After a search of the internets, I found sheet music for these tunes. These will be the “standards” for rallies. They are chosen on the basis of being easy to sing a long with, using the Chants and Songs for a Lively Protest booklet from teh Syracuse Cultural Workers. I did not include every single tune from there; there are also tunes here that came from other traditions.
2. Ain’t Going to Let Nobody Turn you Aroundhttps://youtu.be/WPuBGcng6Tw?feature=shared this is a gospel tune, call-and-answer. Gained prominence during the civil rights era.
10. I will Survivehttps://youtu.be/6dYWe1c3OyU?feature=shared Every Woman I know has memorized these lyrics. 90% of the tune is a riff and the rest is instrumental, equally well-known disco
As most readers know, I am not in Nepal presently. I do not plan to teach there in 2022. I wish everyone the best.
My most recent blog entry was intended as a sort of passing-the-torch to any others that may wish to embark on critical care development in Nepal or any other Low Income Country. I was a bit remiss in not linking to Gradian Health Systems.
This morning I got an email from Gradian Health Systems describing their work to develop and distribute mechanical ventilators to Africa and Asia.
If you go to the Gradian Health Systems website, you will be able to see country-by-country summaries of their activity. Nepal is highlighted in one section.
The email I received included this one-paragraph summary:
“Supporting COVID-19 Response in Nepal
“Gradian, in partnership with the Nick Simons Foundation, the National Innovation Center Nepal (NIC), and the America Nepal Medical Foundation (ANMF), launched a partnership to strengthen critical care services at nine hospitals across Nepal. Over 50 Comprehensive Care Ventilators (CCVs) and 100 oxygen concentrators were distributed to zonal, regional, and teaching hospitals in remote regions throughout Nepal, as well as three central hospitals in Kathmandu including Bir Hospital and Civil Hospital.
“NIC engineers and technicians then installed the CCVs, led biomedical training for hospital technicians, and provided support, with the coordination of Gradian’s clinical training, for providers at the hospitals. Under the leadership of Gradian’s lead clinical trainer in Nepal, Dr. PusparajPoudel, over 150 clinical providers were trained across the nine hospitals using Gradian’s mobile simulation training kits and CCV training curriculum. Of note, Gradian and its partners mobilized this effort within a matter of days thanks to the technical expertise of all three partners in medical technology, clinical practice, and biomedical engineering.
It is easy to sign up for their email list. They have a section devoted to their training resources as well, which I think is pretty good.
Greetings. you have found the blog of CCNEPal, a sort of pseudonym I used when I travelled to Nepal to teach. Over the course of years I chronicled my trips and wrote about the challenges of doing critical care in a low resource setting. There are about 250 blog entries here. Feel free to browse. If it is photos you want, go to the accompanying FaceBook page. I tried to share things I learned in case any other foreigner wished to go on a similar quest to any Low Income Country to conduct training.
It’s time to reflect on the entire trajectory since I did not go there in 2020 or 2021, and unless something radically changes I do not expect to go there in 2022. The pandemic has forced me to reconsider those plans. I wish only the best to all the people of Nepal and South Asia and all countries, but the torch of excellence in critical care is being passed to a new set of players. I think I did the best I could to carry out a quest which was Quixotic at times. Therein lies a tale.
2007, 2008 and 2009
I actually made three trips to Nepal before deciding to focus on critical care and the grandiose plan of changing the perception of the value of such a service. Though I had been a nurse for decades I had not really travelled outside USA much. It had been a lifelong desire to visit India and the Himalayas, and the circumstances lined up to allow me to go in 2006, so I began to plan the first trip.
Tansen
I contacted United Missions to Nepal and arranged to teach nursing in their PCL program in Tansen, Palpa District. Tansen is a small city in the hill country, and Mission Hospital has been there for around fifty years. It attracts a small community of videshi medical personnel who provide mutual support while offering their skills. It was an ideal place to start learning about Nepal healthcare due to this factor of having a peer group. Many of these persons were quite colorful.
View of 2007 Mission Hospital from a viewpoint on the hill above it.
What I learned in Tansen was that the status of critical care was low. Not just in Tansen but throughout the country. There were severe deficiencies in traning and practice. This was not a reflection of Mission Hospital per se, but an outgrowth of decades of priority-setting in which a very utilitarian approach to allocation of resource was followed at most levels. I think I was careful not to present myself as “the kuire expert from away” and to respect the challenges of delivering care while there, but I couldn’t help from seeing examples of excess deaths in the acute inpatient care, due to the way things were set up. I would followup by discussing things with the people around me and there was always an explanation for why it had to be the way it was.
“We only have a fixed amount of money and we need to spend it on areas where it will serve the greatest number of people.”
“‘Our Priorities are infectious diseases, maternal-child health, and public health in general. It’s foolish to focus a lot of money on a small population such as would be candidates for critical care in the west”
In the first year in Nepal I even met a nurse in Kathmandu who was a consultant in nursing ( a Nepali person) who told me I was wasting my time thinking about how they could do better at critical care and it wasn’t needed. In the second year on a teaching trip outside Kathmandu Valley I met a senior doctor who told me that it would be impossible to teach any nurse in Nepal how to read an ecg strip. The mindset was pretty firm.
The first summer in Tansen ( I tended to go only during summer vacation from my University teaching job), was a shock to me. I spent the following eight months trying to recall if anything really actually happened the way I remembered it, or if I was somehow exaggerating past events out of proportion. This sense of puzzlement led me to return in 2008 and 2009. I think many other videshi persons would not have done so, chalking their time up to experience; but I could not move on after having done it the first time.
Outgrowing Palpa District
On subsequent trips I contemplated the idea that Nepal has thirty million people and the one hundred sixty bed Mission Hospital in Palpa district was not going to be a place from which I could make any kind of large impact to teach critical care. So I started to develop contacts with people from other parts of the country, especially Kathmandu the capital. In summer of 2010 I stayed in USA to spend time with my daughters, then returned to Nepal in 2011 with the idea of CCNEPal.
My new home base was Lalitpur Nursing Campus, considered to be the best nursing school in the country at that time. It was still within the archipelago of former projects of United Missions to Nepal and they were used to hosting foreigners. For a nominal fee I could use their largest classroom. The campus of LNC was housed at a former Rana-era palace and it turns out that the largest classroom was the former ballroom, replete with red velvet curtains on a small stage, colorful decor and a large crystal chandelier. I taught four or five sessions of an elementary critical care course, and also took my first trips to Bharatpur and Bhairawaha to teach in Terai. And we were off to the races!
Teaching in a former palace
This is the former ballroom of which I speak. I taught in many venues, but this complex of rooms was the site of about thirty of my 125 sessions over the course of time. The rules to register for classes here were not the same as elsewhere; usually with other hosts they populated the roster with staff that all came from the same host agency. For this venue, each session was first-come-first-serve, advertised on the Face Book page with 7,000 followers. We got a wonderful mix of participants and some sort of synergistic education magic happened each time. Lots of positive vibes here!
NSCCM
There was a very small community of doctors doing critical care in Kathmandu in those days. The Nepal Society of Critical Care Medicine had been formed, but they were small and limited to Kathmandu inasmuch as they did not see themselves as having a national vision that I could tell. This was before the return of Subbash Acharya from Canada where he had done a fellowship in Toronto. The NSCCM did not give much thought to the training needs of nurses in those days. At the time I was dismayed that they too had tunnel vision as to the possible benefits of developing a robust approach.
Fast Forward
The first courses were specifically for nurses in Nepal. I got excellent “word of mouth” and the participants were quick to recognise the value of what I was teaching, often returning to their hospital to lead critical care services and tell others about me. A ripple effect began and grew to a wave. Soon, I was busy teaching two three-day short courses per week when I was there, travelling throughout the country, and developing relationships. This included more time in Terai, the hot southern flat region bordering India. I began teaching session to MBBS students and Medical Officers.
Over the period from 2011 to 2019 I taught 125 sessions of my course, giving certificates of completion to more than 4,500 nurses and doctors. The knowledge was becoming more widespread. My “word-of-mouth” reviews continued to be excellent.
I soon learned a cardinal rule of education in Nepal. There must be a certificate. And it better be nice. There is a story behind this particular photo. It seemed that the Nightingale College BN students were on the tail end of a long road trip, and I’d run out of certificates ( oh nooooooo). I got theirs in Kathmandu and mailed them but they got lost along the way. When we finally found the packet, I told then I needed photographic proof that the certificates had been handed out. Hence this photo. And it illustrates that if you wish to effective in critical care you need to have a sense of humor and irony.
There had been pockets of medical knowledge in this area around the country and those places didn’t need help from me, but the training led to higher standards in parts of the country where they were too far from Kathmandu to get their knowledge from there. One unexpected side-effect of teaching critical care was that I also taught de-escalation techniques to minimize the likelihood of “thrashing,” a related problem. I worked hard to identify specific obstacles and continued to tweak my training as I learned more about specific needs.
During that same period, Dr Subbash Acharya of TUTH became the driving force behind NSCCM. He worked tirelessly to create and enlarge the community of expertise in Nepal, and helped establish the Nepal Association of Critical Care Nursing. Also, I helped organize the first American Heart Association International Training Center for ACLS, run by the Laerdal franchisee Center for Medical Simulation ( CMS), and they started teaching ACLS on a more regular basis year-round.
The pandemic
Those who wish to have more of a blow-by-blow recounting of events will find more detail in the past blog entries. We are now in the midst of a worldwide pandemic of covid-19, and Nepal is among those countries that have undertaken efforts to strengthen critical care. Obviously the first step is to purchase specialized equipment, but we still need to train staff in specialized skills, and this is now ramping up.
Validation
There is so much to say about the time I spent, the learning that took place, and the progress that has been made. Permit me to be smug for just a minute here. All the things I said after my early trips to Nepal have been shown to have been necessary for the advance ment of health care there, and there is a much stronger voice for the teaching and practice of critical care skills, than had existed when I started. Obviously, I was not the only person invloved in this progress. I normally don’t blow trumpets and beat a drum to say how wonderful I am – far from it. But I think I did make a difference with this project.
Gratitude
There are many people ( Nepali and videshi both) to thank for all the time there and the successes we had. Perhaps too many to list. Perhaps hundreds. The best part? once people grasped what I was trying to impart, a wave of enthusiasm was created and we surfed it like being barreled. If I could line them up, I would give each a kata scarf, a marigold garland, and a tika. I like to visualize small tokens of gratitude in that way but the actual doing of such a ceremony would take days – so let’s just call it good. I personally have been enriched by getting to know so may truly dedicated people working against heavy odds to help their fellow human beings. I have loved learning about Nepali culture and I like to think I now a world citizen in a way I would have never contemplated if I had not spent the time there.
As the saying goes, I even loved the parts I hated.
Stay Tuned
In the past I mostly contribute to this blog when I am actually in Nepal. I may still write here from time to time, but I don’t know when. Until then, best wishes to everyone!
PS I will publish this today and edit it periodically to add URLs, photos and the like.
Now is the Time for All Good Nurses to Come to the Aid of Their Country
So we are at the phase where it is “all hands on deck” for those who know how to give an intramuscular injection and also possess free time. Like everything else in the covid19 pandemic, the federal government could have been getting this organized last year while we were waiting for the vaccine, but – they did not. I took some Public Health courses at undergraduate school back in the 1970s and even then it was a well-known axiom that politics and controversy will always accompany every public health initiative you can think of.
I am an RN, over sixtyfive, still working and yes, I have pre-existing conditions that put me at risk. I swear the retired RN who gave me my second shot looked like she was eightyfive years old. The pandemic creates opportunities for retired nurses, it’s the “work until you can’t hold a syringe” employment event. I should add, she had impeccable technique. I told the nursing students with me that they would now have a story they could tell their grandchildren as to what they did during the Great Pandemic.
Nursing ShortageMost nurses who want to work are now employed as nurses already. Here in Tampa Bay, there was an estimate that one thousand nursing jobs were unfilled prior to covid19. This is Florida after all, and older Americans want to retire here. My county in Florida has about 1.5 million residents, and there are eleven entire US states with fewer people to vaccinate.So the school where I teach is now partnering with the County Public Health Agency to allow nursing students to help staff the clinics that are taking place. We send a group of four or five at a time along with a faculty member ( an RN with a Master’s degree or even a doctorate) to a predetermined location to meet the Public Health staff, and away we go.
I actually did it first, prior to the beginning of the semester, and I reported back to my colleagues what it was like so they would have an idea. I was asked to gather teaching resources so the students would be prepared, and so I put together a small list and shared it on our Learning Management Software. (the computer app on which all aspects of college courses resides these days. It’s very different than when you went to school!).I decided to also share the list with my blog, for other nursing faculty who have not yet read up on the details. So, here goes.
The Pfizer “Package Insert.”When nurses learn pharmacology they are taught to make a “drug card” for each medication they administer so they can have a handy reference summarizing what to tell the patient. The Pfizer vaccine came out too recently to make it into the reference books every nursing student is required to buy and study. Here is the source document from the drug company that gives all nursing-related info on the Pfizer vaccine: https://www.fda.gov/media/144413/downloadPlease note that the package insert is thirty pages long. The last fifteen pages include a review of studies related to the drug. I do not require students ay my level to digest that section.
A CDC checklist on vaccine administration for the nurse.
The CDC has many documents and videos etc on their site. One that I thought applied to nurses was this checklist. It was made for the covid19 vaccine but it goes over items needed for all vaccines. https://www.immunize.org/catg.d/p7010.pdf
The seventeen dollar CD
At the top of the above checklist are the instructions for how to buy a CD of all these resources. The DVD “Immunization Techniques: Best Practices with Infants, Children, and Adults” helps ensure that staff administer vaccinescorrectly. It may be ordered online at www.immunize.org/dvd.
Another helpful resource is CDC’s Vaccine Administration eLearncourse, available at www.cdc.gov/vaccines/hcp/admin/resourcelibrary.html. Browse the CDC site. Among other items you will find the meticulously-detailed storage procedure for the various vaccines. As you no doubt are aware, the Pfizer vaccine requires cold-temperature storage until use that adds a complicating element to distribution. They go through it step by step.CDCTrain – CDC developed a training module for health care providers: https://www.train.org/cdctrain/course/1095082/
How to give a deltoid injection
I hate to admit how old I am, but at the beginning of my career, medical care relied on intramuscular ( I.M.) injection for delivery of many more than meds than they do now. Giving a pain shot was a frequent event in any hospital setting. Somewhere along the way, the new standard became to deliver pain meds through the intravenous. It hurts less, there is more reliable absorption, and the patients like it more. These days a student can readily learn to give insulin ( a subcutaneous injection), but does not get as much I.M. practice. In every nursing school, this is part of the curriculum and every nursing student is required to get checked off on the procedure, including passing a quiz and showing a demo of how they would go about it. Every Fundamentals of Nursing textbook describes it in great detail including the basic checklist. However, the injection technique is still worth a review the night before joining a clinic.
There are many YouTube videos on the subject. Here is my favorite: https://youtu.be/DBHnd3N-5Ns Note, “RegisteredNurseRN dot com” is famous among nursing students. They have 1.2 million subscribers, and have produced 762 videos. Her delivery style is excellent and when I have required my own students to make an educational video, some of the groups will create a sort of parody of her delivery. They love her and I think the info she presents is of high quality. ( disclaimer: I am not associated with RegisteredNurseRNdotcom in any way and this testimonial is freely given with no inducements of any kind).
YouTube
We are targeting nursing homes and longterm care facilities first. For these, the administrators provide a list of eligible residents, and collect the consent form. The county plans out the details including where to send the team and the location of the nearest hospital in case of any problem. If the residents can come to a common area they are brought there, but if not, the team will go door to door to find them. The county has a master list of all such locations and has made a systematic plan.
Drive-Through clinics
This has been new. There was an initial learning curve on how to set up a drive-through event for a thousand people at a whack, and it involves a lot more traffic control than you might have imagined. ( most people drive up with one or two recipients in the car. You don’t want to create a bottleneck by taking up a lane on the actual street where traffic is moving!) At the first one I joined, they had about eighty volunteers managing traffic and they set up a pattern using orange cones. So, I included some videos showing what it was like to be part of this. When they hold a drive-through clinic, they need to have a plan for the staff to wash their hands, go to the bathroom, and get lunch. I knew this so I brought some snacks the first day and I think I was the only one. (the organizers provided gloves and about a gallon of hand gel per person). They did supply lunch and a break.
Note: you do not need special training to volunteer as a traffic director. Any reader can phone up the local agency in charge of this and volunteer. They will lend you a reflective vest. Dress appropriately!
Here are some YouTube videos that give an idea of what it is like. You may have seen these on the news. There is a learning curve for the organizers.
I will post this on DailyKOS where I hope people will forward it to any and all Health Care Providers who might be helped by this, but also on my own blog that I usually reserve for entries related to Nepal health care. https://wp.me/p1pDBL-1L6 For those who have followed me, I sometimes have written about the political situation in Nepal, but I did not travel there to teach in summer 2020 due to the pandemic and I don’t expect to go there in 2021 either. In Nepal we frequently discuss the concept and application of the idea of “excess deaths” but it was not something I thought would ever enter into the national conversation here in USA.
One of my personal favorite DailyKOS diaries that I ever wrote was my movie review of Contagion, back along. Was it really nine years ago? I think the review stands the test of time. Let me know.
At my WordPress site you can read about my work teaching both critical care skills and de-escalation skills to Nepali nurses and doctors.
Background, June 7th, 2020. Like everybody else I have been glued to the tee vee as the protests unfold since the murder of George Floyd. I have been appalled by the lack of training and professionalism of the police departments around the country, and we get endless instant replays of improper use of force on protesters who are not a threat to the police. In the past I have spent time learning and teaching about de-escalation, situational awareness, and the like.
If you would rather read it here without clicking, it is shared below in all it’s glory:
Let’s start off by saying this is a niche book.
Really.
IMPORTANT POINT: If you are a mayor or governor or staff policy expert, deploy your state’s National Guard early as opposed to late. The local P.D.s can not be relied upon to have had the kind of training to carry out the procedures, tactics and strategies shown in this book.
Now that we got that off our chest, this book is recommended for all persons interested in the study of communal violence (“rioting”). Obviously on the list are the civil authorities whose job is to prevent injury or loss of property while allowing peaceful demonstrations to occur. Less obvious would be the protesters themselves; and any attorney who would represent protesters harmed by police in riot control actions. Elected public officials need to learn what the training entails and what their own role may be in de-escalating emotions of mass gatherings.
The book is five chapters and covers
Operational Threats;
Control Force Planning and Tactics;
Equipment and Techniques;
Control Force Formations; and
Confinement Facilities. (i.e., special considerations when addressing prison riots and/or extracting an unwilling person from a solitary confinement cell, for which there are specialized teams in Federal and State prisons).
At the back is Appendix B, “Practical Applications,” an innocuous title for one of the truly informative sections of this book. It covers topics such as Negative Indicators of a Potential Civil Disturbance and Prevention of Crowd Escalation. If I were to find fault with this Handbook it would be that this section is not long enough. In the recent spate of protests, the police response in so many cities showed a lack of situational awareness and an inability to grasp a fluid situation. Future issues of this book ( or maybe future companions to this book) should consider more of an emphasis on case studies for the overall strategic commanders.
The book could use a chapter on how to utilize the geographic terrain of a city to deploy troops and shape the movement of crowds.
Because it is a government manual ( “handbook”) and represents the way that the riot control police in USA should be trained, it lays out a set of standards and best practices that serve as a contrast with the way the procedures are actually implemented. The disparity between the standards and the implementation is where a lot of civil suits arise. Due to the massive nationwide protests of May and June 2020 ( which are not over yet as of this writing) anybody with a tee vee has been able to watch riot control as if it is a strange variant on American football. At one level, it is just that.
The book integrates relevant points of law along the way and highlights some problem areas, such as how not to hold a police baton, and how to aim when firing a non-lethal baton round.
Chapter 4 is a bit confusing unless you study the key to symbols on the first page of the chapter, used in the many later diagrams. The chapter covers a variety of formations used to accomplish the dispersal of crowds as well as alternative ways to setup an extraction team in these various situations. This chapter reminds me of the kind of “playbook” used by college or professional football team inasmuch as it depicts the way you would set up the players prior to executing a pass play or a run play or a kickoff. These take time to study before you comprehend the value of each. The book could benefit from a companion DVD or YouTube Channel showing these various formations and tactical problems.
In short, the book is a niche book. It presents the way of thinking of the field commanders for a law enforcement agency. I would predict that it will be revised after we have all had time to stop and reflect. I am in hopes that police and National Guard units from across the USA will use this book and others, for future training so as to avoid the kind of errors they got into during the George Floyd protests.
I had not really looked at the most recent diary on this page until today. Normally I mostly activate this blog when I am actually physically present in Nepal. I’ve linked to some past entries ( especially the one on Rubber Bullets) and I realize people are now finding it and they are wondering Who Is This Guy?
I am an RN and my first trip to teach nursing in Nepal was in 2007. Since 2011 I focus specifically on teaching critical care skills to nurses and doctors there, and I have cycled about 4,300 nurses and doctors through my training courses.
I got dragged into the topic of “Communal Violence” early on. Physical assaults on doctors and nurses is a sad fact of medical care in South Asia and as you might imagine, the fear of injury is an impediment to advanced study of resuscitation and critical care ( understatement of the year). Many of my past blogs address aspects of this. In Nepal I am actually kind of famous (or would notorious be a better word?) for this and my courses are always packed.
Because of the political situation there I have engaged in an informal study of riot police and their tactics. It has helped me make peace with things that have happened along the way.
Normally I would be there right now. The Jacaranda trees are in full bloom. I would have had a quick week in Kathmandu before travelling to the Terai region. But it was not meant to be.
If you look around, you can find links to my two books on Amazon, each of which devotes space to the subject of “communal violence.”
This will be brief. CCNEPal teaches a version of Advanced Cardiac Life Support to nurses and doctors in Nepal. Since inception in 2011 we have trained 4,500 nurses and doctors. ( yes, it’s a large number, hard to believe). We usually spend about eight to ten weeks in Nepal in summertime.
Nothing is ever official until I buy my airline ticket in March or April. But we are beginning to think about activities.
There are certain host agencies and schools we always work with, but each summer we are willing to go to new places to share our knowledge and to consult with the local professionals as to how to do critical care. We tend to work more in the Terai these days.
If you are interested to host us, browse this blog and find previous entries that describe what we need in order to run a successful training. Then send an email to joeniemczura@gmail.com
This is a book review of The Vagina Bible, which finally hit bookstores only a couple of days ago. I posted it on another blgo then figured I would crosspost here.
The executive summary? Get it. Read it. Share it. If you want more details, step over the line.
Who is Jen Gunter, MD?
Jen Gunter MD practices medicine in the Bay Area of California and is a fully Board-Certified OBGYN in both Canada and the USA. For those who do not follow medical credentialling, “board certified” is the gold stamp of approval in terms of clinical expertise. Her official title would be “Jen Gunter MD, FRCS(C), FACOG, DABPM, ABPMR (pain). She explains the meaning of the string of initials if you visit the “about” page of her website. But Dr. Gunter is very approachable and informal and a tad irreverent when she starts talking about her passion — women’s health (which is also “human health” if you think about it).
@DrJenGunter
Dr Gunter’s motto for her Twitter feed has been “come for the sex, stay for the science; come for the science, stay for the sex.” which is apt. Also, “wielding the lasso of truth.”
She is impeccably grounded in the research to support a sound approach to gynecology care, and yet also has a sense of humor that is utterly delightful to a curmudgeon such as myself. She is is a master of the 140-character takedown of those foolish enough to dispute her expertise.
That is what I have decided to name a collective of mansplainers. A murder of crows, a parliament of owls, a rash of mansplainers. In medicine a rash can be a mild annoyance that goes away and never returns. A rash can also portend a serious medical condition, even something malignant.
There have always been a few men here and there explaining vaginas to me. I have suffered fools eager to use pickup lines about being an amateur gynecologist, detailing their imagined superior knowledge of female anatomy and physiology. Men who think sitting beside them at a bar and smiling — because if you don’t smile, you get told to smile — is an invitation to tell you how they will make you scream and moan.
I was already hooked on her writing, but this made me howl with delight. The piece was a manifesto of sorts, and Dr Gunter gained a following that went beyond a mere cult, into the mainstream. Her subsequent skewering of myths and misconceptions promoted by the women’s wellness industry has attained legendary status, especially with her science-based analysis of false claims by GOOP magazine, over such issues as the use of Jade Eggs. These days I don’t think anybody can read the name ‘Gwenyth Paltrow” without also thinking of Dr Gunter and the way her lasso reeled GOOP in.
Book Dedication
The dedication says:
For Every Woman Who has Been Told — Usually by Some Dude —
that she is too wet, too dry, too gross, too loose,
too tight, too bloody, or too smelly.
This book is for you.
The chapters are logical, first starting off with accurate medical information as to anatomy, then going in to childbirth. Then she gives practical advice on such things as lube, underwear, menstrual hygiene, sexually-transmitted diseases, and common complaints or symptoms that bring a woman to a gynecologist for examination. Throughout, she maintains a pro-woman attitude that would make me want to tell me daughters to make an appointment.
Context
In greater context, this book is the next logical heiress to Our Bodies, Ourselves, the famous book by the Boston Women’s Health Collective that championed the revolution toward woman-friendly non-patriarchical women’s health in the 1960s and 1970s. That book went through successive editions that made it larger and larger; the most recent updating was in 2011. My wife and I had a copy of OBOS which we left laying around the house for our daughters to read. Gunter’s book is very readable and rivals the colloquial style of Everything You Wanted to Know About Sex ( but were afraid to ask) by David Rosen, MD, another pop book from the 1960s that was a #1 best-seller of the New York Times when it came out ( and later made into a movie by Woody Allen). (it seems to be out of print).
Political Views
I would be remiss to omit Dr. Gunter’s unerring and consistent defense of a woman’s right to choose; her insistence on framing the abortion debate in medical terms including calling out the lies about “late term abortion” and “infanticide; ” and fighting back against other attempts by radical pro-life extremists to fan the flames of emotion rather than appealing to rational science. I don’t follow the pro-life extremists on Twitter but they seem to flock around Dr. Gunter like moths to a flame. She seems to be a lightning rod for pro-life weirdos and yet she supplies excellent talking points on the front lines of compassionate gyn care. The Vagina Bible is not, however, a polemic book carrying a radical torch. Dr Gunter stays very carefully on the side of science-based advice in all areas it seems to me.
Barnes and Noble
I got my copy in the Women’s Health section of Barnes and Noble here in Tampa. Why it was not yet stacked on a table in a more prominent area of the bookstore was actually a mystery to me, since the topic is of wide interest and the book is well written and factual. Maybe there are just not that many nonfiction best sellers these days. Still and all,this would be a great beach read, the kind of book you could enjoy by just going to a random page.
Twitter Controversy
I should say, this past week there has been a bit of a controversy on Twitter since her publisher wanted to run a series of Twitter ads with the book title but was somehow blocked by Twitter due to the prominence of the word “Vagina.” For those of us who have been following the good doctor, this has been a strange twist. We have a situation where Alex Jones and his ilk can promote lies about such things as Sandy Hook; where people use not just the f-word but also the c-word; and of course a President who lies and also shares top secret national security items that put American lives at risk; and yet — a book written by an MD in which the title describes the subject is somehow off limits? Get real.
Amazon Book Reviews
I shared this review on Amazon, and I was at first surprised to read that there was a one-star review posted by an MD at that site. Turns out, the MD in question has her own nickname – “The Love Doctor” and in Austin Texas she runs the sort of bespoke clinic that promotes just about all the trendy treatment modalities that Dr Gunter is advising against. So – I expect there to be a backlash from proponents of the “Vaginal Shaming Industry” that Dr Gunter is informing us about.
In summary
I give this book an A plus for readability, accuracy and reliability.
Disclaimer
I am not in any way associated with Dr Gunter, or her publisher. I have not received any compensation for this glowing review in any way. I paid for me own copy and I had to wait for it like everyone else!
I am back in USA this week, and next week I resume teaching at a nursing college in Tampa, Florida. The flight from Nepal to USA was uneventful but long. Oh wait – I lost my wallet and one of my bags got lost – but overall it was okay. I would recommend Quatar Airlines to anybody.
I was in Nepal eighty-two days. I taught thirteen sessions of my course, and awarded 317 certificates to nurses and doctors. This was fewer sessions and certificates than past summers where I tended to teach about 24 sessions and got close to 600 certificates each time. I had a number of requests to teach additional sessions that I was not able to fulfill, due to travel requirements or the heat.
CoMS Bharatpur
Most of the sessions were at College of Medical Sciences in Bharatpur. This host agency has an airconditioned classroom which has ample space and they supported conditions that made it easy to feel good about the quality of learning we could provide. My partners there have known me since 2011. They provide fooding and lodging (with aircon!) and they were always upbeat. As in past summers, I note that the students at CoMS are more often from the Terai and indeed to complete their government service in Terai; this is important because Terai needs to work more on outcomes for health than other regions. I think I could walk into any number of subsidiary hospitals in Terai and be greeted by a nurse or doctor who took my course at CoMS. Like all good Universities, CoMS serves as a knowledge node from which expertise billows out.
CoMS was kind enough to allow me to teach a session to nurses and faculty of NPI Hospital and NPI college of nursing. I had previously taught a session at the NPI hospital but in an area that lacked aircon.
I knew it would be hot, but not this hot. My problem is, I can only go to Nepal in summer due to my teaching job. I was asked to teach in other Terai locations, but declined to do so unless there was air con. Also, my highly- anticipated trip to Nepalgunj was postponed indefinitely due to heat, then flooding.
Kathmandu
I taught only one session in Kathmandu, at Bir College of Nursing. The audience was BNS students. These persons are returning for a Bechelor’s Degree. The pathway for them is get their PCL, then work two years and return to school. Most of this group were working in the system of government hospitals, and one of the priorities of the Ministry of health is for the BNS students to focus on critical care skills. So the group was an ideal target audience for me. They were so much fun to work with. I returned there a week later for a daylong session on ecg reading, something I don’t normally do.
Other hosts in Kathmandu
I can legally teach my sessions in Kathmandu because I have an RN license in Nepal. However, there were two other host agencies operated by the government that originally wanted me to teach, then requested me to show a letter from the Ministry of Health to authorize my teaching. This is also a pathway to “legally” teaching, but one which I was told by the Nepal Nursing Council that was not needed by me. So the first plans went nowhere. I am exploring the idea of taking steps to get such authorization from the MoH for next year. There are about thirty hospitals int eh government system trying to upgrade their critical care skills, and I am thinking this might be a good focus.
I returned to Terai for one session, at Bharatpur Hospital. The roster there also included faculty from NPI, and from Balkumari and from Maya Devi College, in addition to the nurse who serves as Regional Burn Coordinator.
My daughter the tourist
The last two weeks of the summer were devoted to tourist activities. My older daughter finally visited me in Nepal and we had fun. She later said how much she loved the people and culture here and that “it was the trip of a lifetime.”
The only festival that take place during monsoon is “Gathamuga” in which the frogs save the world. (more or less). It was so much fun!
The itinerary included three days in Chitwan seeing wildlife and interacting with elephants.
Julie never was in the presence of a loose monkey before this trip.
She also got a kurtha jangrawal at a place in Indra Chowk, and went on a yoga retreat.
The kurtha jangrawal is associated with the Newari cultural group. I think she looks terrific wearing this. Lots of videshis buy a sari or a kurtha, but few have this tailored for themselves.
It was good to stop and smell the incense.
Airway Management Trainer
How could I forget! CCNEPal organized a crowdfunding campaign to donate one of these to CoMS. We made a handover on July 25th.
This training tool will provide education to MBBS students, Interns, Medical Officers, and nurses at CoMS for decades. Because the school sends graduates throughout Terai, it is a resource to improve the technical skills for the entire region.
Time to reflect
I now have six or eight months to think about how CCNEPal can help advance the practice of critical care in Nepal. I will be thinking of ways to move the project forward in future years. I expect to decide about the 2020 trip in March or April, then send out an announcement as to available time slots and sessions in April or May.
Swasthya Khabar needs to stop attacking and start helping
So there has been a series of newspaper articles in Swasthya Khabar that investigate issues within the nursing profession of Nepal. These have been written in Nepali language, and I start by admitting my Nepali is poor. I use Google translate to get the idea of what they are saying. I think these articles are prompted by the recent results of the nursing licensure exam in which only about a third of nursing college graduates achieved a passing score. Also, there is a desire to use the press as a way to develop public opinion for a plan that will guide further development of nursing as a worthy profession in Nepal.
Outside a nursing college classroom in Kathmandu. In Asian culture, shoes are removed before entering a room.
Naturally the general public needs to learn about the best way to proceed and that is a noble goal to guide the Nepali press in a democracy. All Nepali families wish to support the success of their younger members, and many young persons see the possession of a nursing degree as a ticket to employment in a Nepali hospital or as a vehicle to go abroad and see the world while sending remittance home. They can do this while serving humanity. There is nothing wrong with these aspirations.
Graffiti from the stairwell of a nursing college in Kathmandu. Nursing students often live in a hostel fro three years while studying. The curriculum is regimented and disciplined. Families often accrue debt to send their daughter to nursing college.
नर्सिङ शिक्षामा मनपरी : यी ९३ वटा कलेजका आफ्नै अस्पताल छैनन्
स्वास्थ्य, शिक्षा मन्त्रालय, काउन्सिल, सिटिइभिटी र विश्वविद्यालयकै कर्मचारीको मिलेमतो
This is devoted to a discussion of how many of the nursing colleges in Nepal are associated with a hospital. Oh My God! Ninety three are NOT! Now, the fact is, most major hospitals in Nepal operate their own nursing college in the first place. But there are colleges that would be called “free-standing” if they were located in the USA. In fact, the vast majority of nursing colleges in the USA are “free-standing” and it does not hurt the nursing education offered to students in USA.
The reader is invited to look at the Swasthya Kahbar article. I have written a long comment at the bottom, which I will repeat here, edited to improve formatting:
Here is my specific reply to the article in Swasthya Khabar:
(begin quote) This article has strayed from the real issues in nursing education planning. The direction of the article is to accuse all the 93 nursing colleges of breaking the law and suggesting that these colleges need to be penalized. ( and the list of offenders is included, implying that the leaders lack integrity. Are they trying to shame the colleges or would they do better to find a solution?) That is not the way to proceed.
First, it is simply ridiculous to suggest that any nursing college now open their very own hospital with all that it entails. Will the Campus Chief of each nursing college suddenly become a hospital director, employing Medical Officers and Surgeons and operating an Emergency Room and Operating Theater? That idea in itself is ridiculous – of course not. We already have a situation where any group of doctors that can pool their money to build a “hospital” can do so, without any real planning or oversight by any level of government. Why adopt a policy that requires more building construction without consideration of hospitals that already exist nearby?
“Affiliation Agreements”
In USA, it is the general practice for colleges of nursing to operate independently from owning their own hospital, and this would be okay for Nepal too. Of course, in USA each school is required to have an arrangement with the nearby hospitals to allow their students to go there to learn how to take care of patients. Nepal would do well to adopt that approach. A hospital needs nurses, but staff nurses are expensive because to be paid, so it is typical for many of the hospitals in Nepal to start their own nursing college. The labor of the students substitutes for the paid labor of staff nurses. This is a lesson in “economics 101.” In USA these agreements for students to serve at hospitals not owned by their school are called ” affiliation agreements” and the existence of such an agreement should be the proper subject of investigative journalism, not whether the college owns their own hospital.
A better way to explore the issues in nursing education
If you are searching for ways to inform the public about ways to improve nursing education in Nepal, you might consider other areas of reform, such as rewriting the PCL curriculum; re-assigning the development of the PCL program to the Nursing Council and not CTEVT; establishing a higher level of education as a requirement for entry to nursing college in the first place; reforming the overall education system to support women who wish to study science topics; re-assessing the nurse license exam so as to reflect better measuring techniques, and the like.
As for me, it’s true that I am a videshi, but I write a lot about nursing education in Nepal since twelve years. You are invited to read my blog, http://www.joeniemczura.wordpress.com . Now, there are areas in which nursing education in Nepal can improve, but this article is simply not helpful in describing what those areas may be. Anybody who wishes to discuss this with me is invited to find my blog and make a comment. (end quote)
Does that make any sense to you?
I do think the concept of affiliation agreements is already part of the system being described, but there seems to be selective choice to focus on some other idea in the current situation, and I think the focus needs to be maintained on the quality of education, not the presence or absence of a shiny new building that lacks a reason to serve the public.
Over the past eleven years I have watched others come to Nepal to try to teach something, and not succeed. Maybe they don’t assess the audience before preparing teaching methods, or maybe they overestimate the English language comprehension, or some other unexpected issue. There is a long list of pitfalls. We assume an expert clinician somehow knows how to teach.
This is not limited to westerners trying to teach. I recently spoke with a Nepali doctor who decided to teach the nursing staff a new skill by assigning all of them to read a certain book in English, after which he would administer a written test. Yes, that might have worked in Medical College, but it’s not the best strategy for nurses.
I am not an English teacher, I don’t teach English per se. I teach content related to cardiac resuscitation and nursing, to classrooms of people who can speak some English. The people in my class sometimes possess excellent English proficiency and sometimes very little at all. It is not my goal to make them speak English, but the goal is to help them do better resuscitation using critical care skills.
Having said the above, I do find that my background in teaching ESL students is very handy. Look at it this way: I
The View from the front of the classroom.
n Nepal I am always teaching an entire class of ESL students. Many of them already speak Nepali, and Hindi, and perhaps a third language such as Newari or Maithili, prior to taking up English.
“You can be excellent at this even if you speak no English”
My own list:
start off by going around the room to determine the English language level of each person present.
speak in English using the grammatical structure of the local language especially if it is an Asian language.
learn a few phrases in the local language and especially learn the top ten body language gestures used by the host culture.
don’t use PowerPoint but do use a Whiteboard
don’t use vocabulary words longer than two syllables
stop and define specialized words
don’t speak more than three sentences at a time
don’t bring a pile of handouts
do have a FaceBook page for the class that helps people learn in advance what will happen in class.
build in class activities for small group discussion about the content in the local language
think of an exercise or game to accompany each little segment of learning.
assign the better speakers to buddy up with those who have less comprehension
I gave my off-the-top-of-the-head list above, but there is already a lot of material out there. Here is a list of URLs I found useful
https://www.fluentu.com/blog/educator-english/esl-teaching-methods/ I thought this one was terrific inasmuch as I already use many of these techniques! My sessions rely heavily on simulation and use of medical equipment like Bag-Valve-Mask devices and cardiac monitors.
For nurses who teach overseas, I think there is some expectation that somehow they will return a wiser, more well-rounded person with deeper understanding of the human condition and a more articulate way of expressing the universal truths of life on earth. This idea of examining your own assumptions of teaching and learning is a prime vehicle for that realm of self-discovery.
Two-thirds
failure rate on June 2019 Nursing License Exam
The recent pass rate for the Nursing License Exam in Nepal was 35% announced in July. In other words, 65% of the examinees failed the exam. The exam is a two-and-a-half-hour paper and pencil test with multiple choice questions in English, and while the scores are not released, the test-take must answer at least 50% of questions correctly. A sample of typical questions on the exam can be found here: https://www.slideshare.net/rsmehta/nepal-nursing-council-licencing-exam-mcqs-sample These sample questions were published around the time of the 2012 exam.
The announcement about the exam from the Nepal Nursing Council
The vast majority of women enroll in Proficiency Level Certificate (PCL) programs, and there are eighty such around the country. You can enroll in PCL even if you don’t pass the SLC exam. The SLC is referred to as “the iron gate” and these days about 20% do not pass. This is better than it used to be. In other words, after passing tenth grade at the age of sixteen a girl can enroll in nursing school here. She could graduate at the age of nineteen.
If the nursing exam was constructed
by the same people who were in charge of the old SLC exam, that is a problem.
The SLC mindset was to disqualify everyone, not to really measure anything. Any
good teacher soon learns that it is easy to construct an exam that nobody can
pass, not even themselves.
During the time of the Constituent
Assembly, the Nursing Council attempted to institute a system of regulating the
establishment of new nursing programs, but they were over-ruled in a dramatic
fashion when a different political party came to power. The government took
control of new nursing programs and loosened the requirements to start a PCL
program. At the time, the Nepal Nursing Council leaders were replaced. There
were rumors that money changed hands.
Population
Boom a Factor
Now, to be fair, the government had
a problem at that time, which was how to provide a career path (other than
homemaking or shopkeeping) for young women, since there are so many young
persons in Nepal. There has been a “baby boom” and to create the
future, jobs must be created. PCL nursing was proposed as one avenue to prepare
girls from the village for hospital work. Often, the government advisors did
not really have an understanding as to the responsibilities of nurses and the
knowledge base required. In about 2013, I recall attending a lunch with an
American anthropologist and some women’s advocates who were in favor of
relaxing the standards of nursing education mainly to give employment, heedless
of any academic requirements. They wanted to create lower levels of health
workers that would not be as stringent as nursing education. They failed to see
that this was a step backwards, not forwards.
Previous
Problems
The high failure rate of the licensure exam is not a new thing. In 2014, the first year it was implemented, there was an outcry due to the failure rate. At that time, I wrote in my blog that I believed the minimum education prior to admission to nursing school should be “SLC plus two” – meaning that an additional two years of science education should be taken, and thereby increasing the age at which a woman is admitted to nursing school, to eighteen with a resulting higher maturity level. At the time, B SC programs were just coming into existence in Nepal. There has always been a paradox in B Sc nursing education. Nurses trained at the B Sc level are less likely to be subservient to doctors and are trained to speak up on behalf of the patient. At many hospitals, doctors perceived them as a threat and resisted hiring B Sc nurses since they were more likely to advocate for holding the doctors to a higher standard. In those days fewer women attended MBBS programs. B Sc education needs to be covered in a separate blog.
I have written about nursing and
nursing education issues in Nepal since 2011 on this very blog, and you can
browse the 270 previous entries to see the general focus of my work. I first
came to Nepal in 2007 to teach at Tansen Nursing School ,a PCL program in Palpa
district.
There has not always been a licensing exam for nurses in Nepal. This was started around 2012, partly because the International Council of Nurses pressured the Nepali government to comply with international standards for nursing education so as to promote the portability of a nursing education across national borders. In other words, without adequate credentialling, a nurse who moved to another country from Nepal would be required to take their nursing education all over again from the beginning before becoming eligible for licensure in a new country.
At the PCL level it is not uncommon
for the nursing faculty to only have a PCL degree themselves and be only a few
years older than the students. There are fewer role models. This has been
changing but not quickly enough.
Which
Language to use for exam?
Now, the language of instruction and
the language of the textbooks is an issue. Most textbooks are written in
English, and supposedly the language of instruction in nursing is English. The
licensure exam is in English. This presents a variety of problems. First, even
if the textbooks were in Nepali, Nepali is not the first language of many of
the students and it would not be feasible to write editions of each book in,
say, Maithili or Bhojpuri. Next, despite the official language of instruction
being English, there are commonly accepted ways to work around this, and these
exist throughout all levels in the Nepali system of education, form the very
beginning. Many schools use the least amount of paper for their students and
rely on memorization.
How
people study in a resource-limited environment
In nursing, nobody can afford to buy a personal textbook; libraries are not amply stocked, and the jargon of medicine and nursing is difficult to learn ( this is true even for American nursing students). There is a lot of highly specialized vocabulary. Nobody studies “alone” – they study in groups. In other words, five students get together, the best English-speaker reads it out loud, and they discuss it in Nepali to gain comprehension. In the cities more students own a laptop but this is not the case everywhere.
There is nothing wrong with Nepali language
Use of Nepali bhasa is actually close to what it should be. This is Nepal; the patients speak Nepali; the nurses will work in Nepali language to meet Nepali health needs. But there is tremendous variability of English language proficiency across the country. If you meet a nursing student in Kathmandu who is fluent, do not think that they represent all nursing students everywhere. In my classes that I teach, I start each session with a quick survey of language ability since I lecture in English.
I looked at the sample question in the link above from 2012, and I would say that these do not reflect what we would call a “nursing focus” in USA. In brief, the questions rely too much on nurse’s vocabulary and not on the actual decisions a nurse would need to make. In USA there are many examples of the type of question that would appear on the licensure exam. Dozens of sites showing sample questions can be found by Google. For that matter, the National Council of State Boards of Nursing in USA publishes their own test map, and it is very very different than the one for Nepal, being “concept based.” My experience constructing exams in USA tells me that none of the questions in the 2012 sample would be acceptable. Also, when a nurse struggles with language, is it reasonable to impose a 180-minute limit on the exam? Are there numbers available as to who was unable to complete the exam in this time?
So, the exam results leave many
questions unanswered, starting with the validity of the exam, the way it is
delivered, and the way it is used.
Please feel free to share, and to comment below. I invite feedback on this blog, especially if it will improve accuracy. If you wish to give feedback but are reluctant to speak publicly, send an email to me at joeniemczura@gmail.com
Next Blog?
Also, I will add another blog on the topic of what I think needs to be done. Stay tuned.
This will be brief. I wrote a piece on my other blog that describes how to use the settings feature of YouTube to improve your language skills before taking NCLEX, or starting nursing school in USA.
I have found that my tips for Nepali nurses who want to go to USA are read all over the world, not just Nepal. This one is also likely to appeal to a wide audience.
CCNEPal completed session number eleven yesterday with 38 students from the BNS and BMS program at Bir Nursing Campus. This was the third time I have worked with that school and I appreciate the people there. Since the earthquake they are in temporary space at Gaushala, the neighborhood inside the ring road, just south of Pashupattinath temple. Part of our space was a nice verandah but I was cautioned not to leave any equipment lying around loose, because they often get daily visits from members of the Pashupattinath monkey troupe, known for being aggressive. I am trying to picture exactly what a monkey might do with a Bag–Valve-Mask but my mind goes blank. Never make eye contact with a wild monkey.
Three intense days of resuscitation practice culminating in a final exam where each of the groups had to tackle a megacode scenario. As part of the props of the course, I own five black topis. For some reason it seemed like every person in the group needed to get a photo of themselves wearing one.
This brings the total of certificates to 279 nurses and doctors. If I were to continue on this pace I would be in step with a final total of about 600, which has been what I accomplished in each of the last two years.
The campus includes two floors of hostel rooms. About six to a room. Those are mosquito nets hanging from the ceiling. I asked some students to take this for me and they obliged. This is not the same as a “typical dorm room” in USA.
Almost all of the students in the BNS batch seemed to be nurses already working at government hospitals in outlying districts. They plan to return to the outlying districts after completion. This is because they are doing the schooling with loans that will be repaid by service at a government hospital. What this means for me is that Bir Nursing Campus is a fine location for this training. The nurses who took it here will bring their new skills and knowledge of the training approach, to districts in far reaches that I would be unlikely to visit.
At Bir we did the anatomy lab. This is a very short video showing one of the maneuvers we display.
I was told that the group at Bir are given a specific concentration in critical care nursing, the only such one in all of the government system of nursing campuses. I don’t think I understood this until now. That makes me twice as happy to have trained them with my course!
Upcoming schedule
My time in Terai was jampacked with teaching, a choice I made. Ten sessions in five weeks. I am proud of all I accomplished. But now I am back in Kathmandu and I have decided to take a week off and focus on school work for fall semester.
People ask how I manage to get people doing megacode as much I do. My scheme is to divide the usual class of thirty into five groups of five, and designate five others to be my “assistants” for the class. The group helps me choose the “assistants.” I teach mostly in English, but when each assistant gets with a group, they conduct the scenario in Nepali and coach the class members in Nepali. In any given batch, they make it come alive and my course manages to avoid falling into the “one more videshi with a powerpoint and lots of handouts” trap. The engagement is nonstop and energetic. These guys were the assistants at Bir Nursing campus.
Monsoon
Monsoon is due to start any day now, after a few false alarms. I think we could use the rain.
I am in Bharatpur Nepal teaching critical care skills as before. My partner here is the College of Medical Sciences, a well-established medical college that supplies doctors and nurses who will practice throughout the Terai region. I met with them to discuss the training needs, and the Chief of Anesthesia told me he really wished they had an Airway Management Trainer, because he has many people to train on endotracheal intubation ( putting a breathing tube down the throat of a person). It is not an easy skill to master, and there is a conundrum: how do you learn to do this if you are doing it for the very first time on an actual person?
The answer: You need a simulator! Most medical schools, nursing schools and paramedic programs have these in USA, and the student gets time to go through the micro-techniques as many times as they like with no time pressure, when learning.
This is what an Airway Management Trainer looks like. This one is from the Laerdal company and is considered to be the best.
Okay. These are not cheap, and they are not readily available in Nepal.
Here is a fourteen minute description of the set of skills you can learn using the exact brand of simulator we want to get: https://youtu.be/ZJtFb7lGPic
I think after you see the video, and think about it, you can see why this is an important skill to teach using a simulator!
I am presently in Bharatpur at “Purano” Medical College, and I just finished the seventh session. As of June 6th, there are 193 certificates awarded.
the class size is thirty. At CoMS we had one batch of 39. Half were MBBS and the other half were BDS. The MBBS group is finishing their program; in one month they take their last exam as an undergraduate then begin their internship year. It is perfect timing for them to be exposed to this skill set. Conscious sedation is used by dentists in Nepal, and so it is advantageous for the BDS group to learn the skills of this course.
Remaining Sessions in Bharatpur
8) June 9th, 10th & 11th h last three-day session for nursing staff at CoMS
9) June 12th, 13 &14th additional session in Bharatpur, for staff nurses and B Sc students of Zonal Hospital and NPI Hospital.
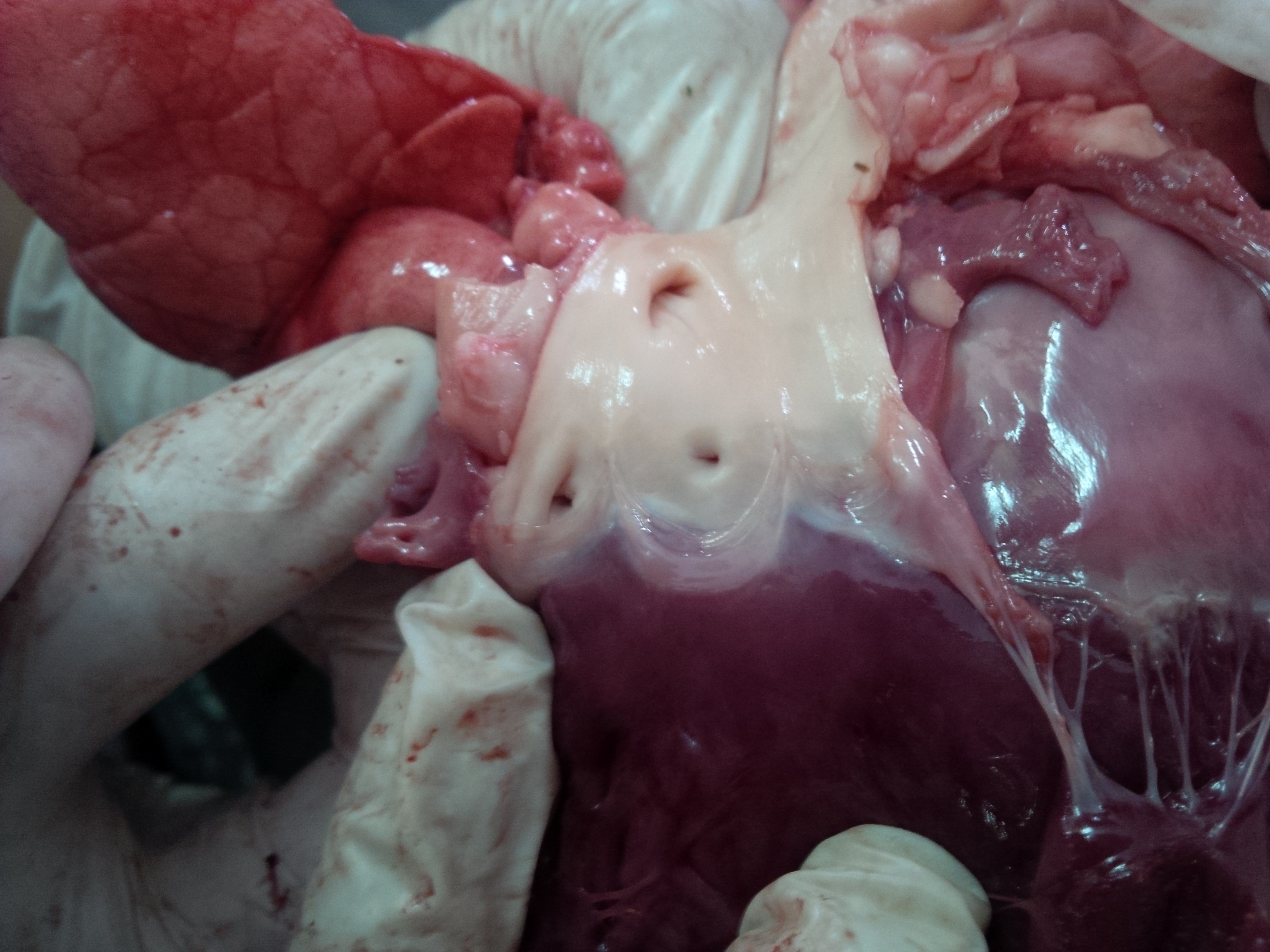
B Sc students in anatomy session of course. For this, we obtain some heart-lung assemblies of goats from local fresh shops and examine cardiac and pulmonary structures. In critical care, it is necessary to visualize what id going on inside the person, (without opening them up to look!) No matter how many books you read or videos you may watch, there is no substitute for examining and handling the actual organs.
Due to the heat and lack of aircon venue I will not be teaching in Butwal this summer, though I love the people there. I will go at some future date during a time of year when temperatures of 40 C are not expected.
June 16th, 17th Last 2-day session at CoMS for MBBS, BDS, Medical Officers
June 18th ( travel days back to Kathmandu and re-settling in location.
June 19th, 20th and 21st National Trauma Center training hall. Three day session for BSc nursing students of Bir College of Nursing )
“Doctor Rajasthani” appears at every session of this course. We do role play and acting. Doctor Rajasthani is the “Senior Doctor” who provides guidance and wisdom when it is needed the most. As for the puggri? we all need a costume. This one was purchased in Jaiselmer, Rajasthan in 2014.
Dates available in Kathmandu are:
June 23rd, 24th and 25th;
June 26th, 27th & 28th;
June 30th, July 1st & 2nd; ( possible at B Sc program in Kathmandu)
July 3rd, 4th & 5th.
Nepalgunj in July
I have always wanted to offer this training in western Nepal but the furthest west I have been was Rupandehi District. I will probably use airplane to get there and back. The weather may impact the final plans and dates.
July 9th and 10th – two -day course for MBBS and Medical Officers (thirty seats)
July 11th and 12th – two-day course for MBBS and Medical Officers (thirty more seats)
July 14th, 15th and 16th – three day course for nurses, especially critical care nurses ( thirty seats)
July 17th and 18th – final two-day session for MBBS and Medical Officers. (thirty seats).
Location – not yet finalized in Nepalgunj.
After July 19th my daughter from USA will join me here and we will do touristy activities.
How to host a training session with CCNEPal summer 2019
Contact me by sending email to joeniemczura@gmail.com
I will travel to locations outside Kathmandu if the host can do the following:
provide a class space suitable for the program. This needs to be a big space. We move around a lot during this class. It needs: 1) a whiteboard (I do not use PowerPoint) 2) thirty chairs, 3) five patient beds or trolleys for the role play scenarios. 4) air con if possible. The classroom needs to be away from a patient care area. ( we make a lot of noise).
provide a roster of thirty nurses and/or doctors or MBBS students for each session of two, or three days. Nurses take a 3-day sessions and MBBS take the 2-day/ Each participant must attend all sessions of the same class to get the certificate (in other words, the three day class is a three day class – not three one-day classes). arrange for morning chiya and lunch, if there is not a cafeteria.
The sessions are for PCL nurses, B SC nurses, or MBBS. I do not register ANMs in the class. It’s okay if the person is a recent graduate, but the persons need to be working in acute care or intending to work there.
while at a place outside of KTM Valley, the host provides fooding and lodging. I live simply, it can be at a guest house, no need for finest hotel in town. I eat DBT etc so I’m okay with local food. At some locations, they lodge me in a private room on cabin ward. ( they do not need to check my vital signs though!)
My preferred schedule is to teach six days per week, either two three-day sessions (for nurses) or three two-day sessions (for doctors). I travel on Saturday and repeat. In summer 2016 I stayed two weeks in Pokhara, two in Bharatpur, two in Janakpur, and three in Biratnagar before returning to Kathmandu.
I try to make a “circuit” of sessions, not go out-and-back from Kathmandu all the time. It’s more efficient.
I supply the certificates. I keep a minimum amount of photocopy but we need about six pages per person.
My Nepali is poor ( I am ashamed to admit). Strange as it may seem, that is not an insurmountable obstacle if there are some English speakers. I adapt my teaching techniques so as to “Code Switch” in a certain way. If a person has no English, this may not be the class for them.
I am presently in Bharatpur, finishing up the 3rd session of the summer. This week it was three groups of MBBS for two-day sessions. I will be here another three weeks.
Remaining Sessions in Bharatpur
4) May 26, 27 & 28 three-day session for nurses and/or nursing students.
5) May 29, 30, &31 three-day session for nurses and/or nursing students.
6) June 2 &3; two day session for MBBS and Medical Officers.
7) June 4 & 5; two day session for MBBS and Medical Officers.
June 6th & 7th 2-day session for MBBS and Medical Officers
8) June 9th, 10th & 11th h last three-day session for nursing staff at CoMS
I am exploring the idea of going to Birgunj for a week or two; this is not final.
I have been requested to return to Bir Hospital College of Nursing for two 3-day sessions. I loved that group during my two previous visits there, and I deeply respect the mission of Bir Hospital; this is also not final
Dates available are:
(please note: because I am already in Terai I would prefer to add sessions in Terai. It’s less bus travel for me)
June 12, 13 & 14th – 3-day
June 16th, 17th & 18th ( three-day)
June 19th, 20th and 21st ( three day)
June 23rd, 24th and 25th; (maybe Butwal?)
June 26th, 27th & 28th; (maybe Butwal?)
June 30th, July 1st & 2nd; ( possibly at Bir)
July 3rd, 4th & 5th. (possibly at Bir)
Nepalgunj in July
July 9th and 10th – two -day course for MBBS and Medical Officers (thirty seats)
July 11th and 12th – two-day course for MBBS and Medical Officers (thirty more seats)
July 14th, 15th and 16th – three day course for nurses, especially critical care nurses ( thirty seats)
July 17th and 18th – final two-day session for MBBS and Medical Officers. (thirty seats).
Location – not yet finalized in Nepalgunj.
After July 19th my daughter from USA will join me here and we will do touristy activities.
How to host a training session with CCNEPal summer 2019
Contact me by sending email to joeniemczura@gmail.com
I will travel to locations outside Kathmandu if the host can do the following:
provide a class space suitable for the program. This needs to be a big space. We move around a lot during this class. It needs: 1) a whiteboard (I do not use PowerPoint) 2) thirty chairs, 3) five patient beds or trolleys for the role play scenarios. 4) air con if possible. The classroom needs to be away from a patient care area. ( we make a lot of noise).
provide a roster of thirty nurses and/or doctors or MBBS students for each session of two, or three days. Nurses take a 3-day sessions and MBBS take the 2-day/ Each participant must attend all sessions of the same class to get the certificate (in other words, the three day class is a three day class – not three one-day classes). arrange for morning chiya and lunch, if there is not a cafeteria.
The sessions are for PCL nurses, B SC nurses, or MBBS. I do not register ANMs in the class. It’s okay if the person is a recent graduate, but the persons need to be working in acute care or intending to work there.
while at a place outside of KTM Valley, the host provides fooding and lodging. I live simply, it can be at a guest house, no need for finest hotel in town. I eat DBT etc so I’m okay with local food. At some locations, they lodge me in a private room on cabin ward. ( they do not need to check my vital signs though!)
My preferred schedule is to teach six days per week, either two three-day sessions (for nurses) or three two-day sessions (for doctors). I travel on Saturday and repeat. In summer 2016 I stayed two weeks in Pokhara, two in Bharatpur, two in Janakpur, and three in Biratnagar before returning to Kathmandu.
I try to make a “circuit” of sessions, not go out-and-back from Kathmandu all the time. It’s more efficient.
I supply the certificates. I keep a minimum amount of photocopy but we need about six pages per person.
My Nepali is poor ( I am ashamed to admit). Strange as it may seem, that is not an insurmountable obstacle if there are some English speakers. I adapt my teaching techniques so as to “Code Switch” in a certain way. If a person has no English, this may not be the class for them.
Many of you know that I also write occasionally for a USA blog named “DailyKOS” – it’s a blog with a million subscribers. It’s focused on electing political candidates from the Democratic Party. But since it’s so big I can reach a larger audience when I post there.
Since 2011, CCNEPal teaches critical care skills to nurses and doctors. Sessions have been conducted in Kathmandu Valley, and also in Dulikhel, Biratnagar, Janakpur, Bharatpur, Butwal, Palpa, Pokhara, and Bhairawaha. We have logged more than 120 sessions and given about 4,000 certificates. But until now, we have never been to western Terai.
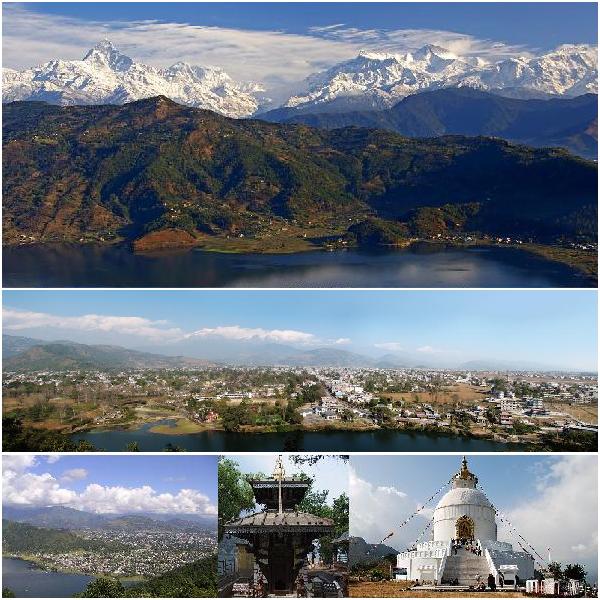
Dr Binod Karn of Nepalgunj Medical College invited CCNEPal to teach at the medical college in Nepalgunj. We accepted the invitation. Hooray! Nepalgunj is a shining jewel of the western Terai!
The teaching hospital of the Medical College in Nepalgunj
July 9th and 10th – two -day course for MBBS and Medical Officers (thirty seats)
July 11th and 12th – two-day course for MBBS and Medical Officers (thirty more seats)
July 14th, 15th and 16th – three day course for nurses, especially critical care nurses ( thirty seats)
July 17th and 18th – final two-day session for MBBS and Medical Officers. (thirty seats).
Location – not yet finalized. the hosts are exploring the idea of using a resort or banquet hall as the classroom. We need a large space.
Because this is the first time CCNEPal will visit the region, we hope that the participants will come from a range of hospitals and agencies.
To register: as of this writing, the roster will be populated by Doctor Karn. His email is drbin2007@gmail.com and inquiries as to available seats should go to him. It is possible that Medical Officers from outside the medical college can also register. Stay tuned for further information.
There is ample information about the content of the training, on this blog as well as the FaceBook page for CCNEPal and the YouTube channel.
We use a scenario-based approach with lots of role play:
these are staff nurses from a Kathmandu Hospital and the scenario is based on USA training methods for critical care.
We start with teaching CPR and basic response:
We don’t use manikins.
we teach people how to use a defibrillator:
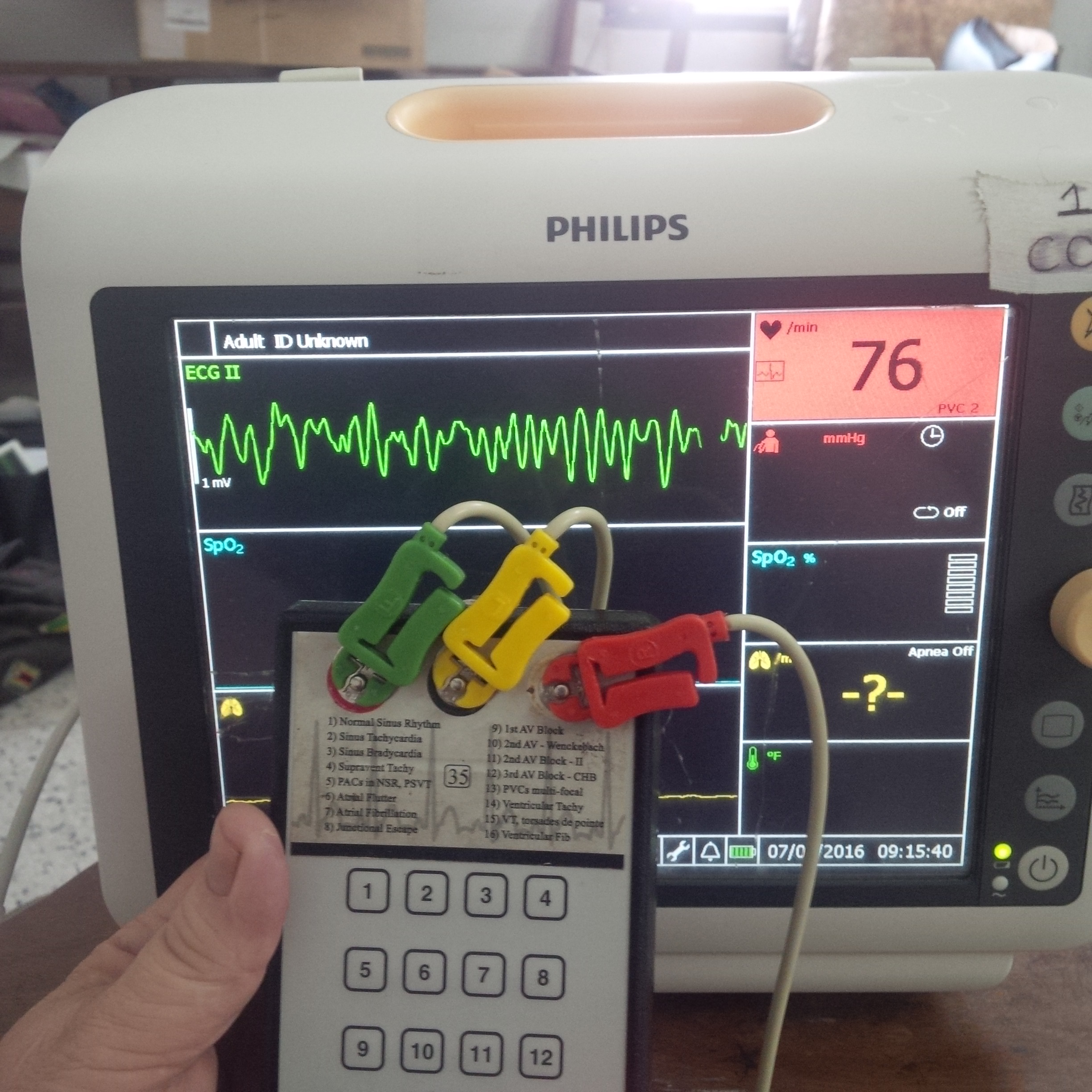
We have one rhythm simulator, and we teach three different practical ways to use ecg in an emergency:
No matter which language you use, the ecg is the same throughout the world.
Feel free to browse the resources. Feel free to share this with any persons you know who are practicing in the region of Nepalgunj!
As previously announced, CCNEPal will be in Bharatpur at College of Medical Sciences (CoMS) for about six weeks in a row and we will offer sixteen sessions of our critical care course. For nurses, the course is three days in a row. For MBBS the course is two days. Most of each batch will be staff from CoMS, but we will also register doctors and nurses from other hospitals or health posts. (see below for instructions).
One of the batches of CoMS nursing students from a previous session. This is a BSc program and the group was enthusiastic and wellprepared.
This is a large air-conditioned classroom that can seat a maximum of thirtyfive participants. Our plan is to fill each roster with that number.
The session is very active. We sit and takes notes and discuss; then we go to beds in the back to do role-play of each scenario. We are fortunate to have a large classroom with air con. You will learn teamwork and communication skills in addition to the protocols. students really enjoy the “Hands on” practical focus. We use the protocols of the American Heart Association as adapted for Nepal.
The dates are as follows:
May 19th & 20, 2019 – two day session for MBBS and Medical Officers.
2. May 21st & 22nd; two day session for MBBS and Medical Officers.
3. May 23rd and 24th two day session for MBBS and Medical Officers.
4) May 26, 27 & 28 three-day session for nurses and/or nursing students.
5) May 29, 30, &31 three-day session for nurses and/or nursing students.
6) June 2 &3; two day session for MBBS and Medical Officers.
7) June 4 & 5; two day session for MBBS and Medical Officers.
8) June 6 &7th two day session for MBBS and Medical Officers.
8) June 9, 10 & 11th; two day session for MBBS and Medical Officers.
9) 12,13 & 14th three-day session for nurses and/or nursing students
10) June 16,17 & 18; three-day session for nurses and/or nursing students
11) June 19, 20 & 21 three-day session for nurses and/or nursing students
12) June 23,24 &25; three-day session for nurses and/or nursing students
13) June 26, 27 &28th three-day session for nurses and/or nursing students
14) June 30 & July 1 two day session for MBBS and Medical Officers.
15) July 2 &3; two day session for MBBS and Medical Officers.
16) July 4 & 5 two day session for MBBS and Medical Officers.
At the end of the session there will be a certificate for those who pass the final exam.
How to register
a. If you are a CoMS student or employee, your in-charge or faculty member will pick the date and assign it to you. CoMS personnel will be the first priority. If you are among this group, you do not need to do anything else. Just show up on the assigned dates.
b. If you are a student from another college or employed as a Medical Officer or Staff Nurse, check with your own campus chief or your in-charge. If such persons register in groups of four or five and the campus chief guarantees that all the slots will be filled, the names of group members will be sent to CoMS. You must attend all three days; actively participate; and pass the final exam to get the certificate.
c. If you are an individual Medical Officer, nurse or health assistant, you must pay a fee of 500 nrs to register. The fee will be used to defray the cost of aircon. We will not accept telephone registrations. You will forfeit the fee if you do not attend – there will be no refunds. We do not accept ANMs in this class.
Contact person for all the above: Dr. Dipendra Khatiwada, Department of Community Medicine, College of Medical Sciences. email is: dipendra.khatiwada@gmail.com and the phone number is: (to be announced).
When you register, be sure to tell us your name; the number and dates of the session as listed above; whether it’s the two-day or the three-day; and how many persons. Include your contact phone number and email. If you are paying the fee in person go to the Department of Community Medicine at CoMS.
Bring: a pen drive. Wear comfortable clothes. Meals are not included with the program but there are many kitchens nearby. classes start at 0900 and end at 4 PM.
CCNEPal offers a threeday course in critical care skills to nurses of Nepal since 2011. Browse past blog entries on this site to learn about our activities.
As of January 2019, the plan is to arrive in Nepal around May 11th. We will spend time running around Kathmandu for a few days then head to the Terai.
From about May 16th to June 30th we will in Bharatpur, Chitwan “The Medical City of Terai.” We will be based at College of Medical Sciences (“CoMS” also known as “Purano”) in their dedicated classroom and offer about 16 sessions. (yes, sixteen). This is the best classroom we have ever had in Terai.
New Registration Option for Outside Participants
In the past, when CCNEPal has been hosted by a large organization we limited the seats to just the persons from the host organization. This meant we did not always have a consistent class size, and the managers strained to accommodate all the requests from staff while still running the wards. CoMS is eager to solidify their status in providing continuing medical education for the region. In summer 2019 we will reserve five seats per session ( possibly more) for nurses or doctors not affiliated with CoMS. This will allow people from District Hospital, NP Hospital, Cancer Hospital or CMC to send a few nurses or doctors at a time to enroll, for example. It becomes easier to continue to staff the units when a few people at a time go off for training. CCNEPal is excited to have this arrangement. To reserve those seats will require a small cash deposit at the time of registration. We have not yet worked out the specifics as to who to contact to register. We will not accept phone-only registrations or email-only registrations.
We expect to teach other sections of our course in July, possibly as many as six. On a recent blog entry, we described the requirements to host us.
Ten Rules for the Flipped Classroom
in Nursing School
By Joe
Niemczura, RN, MS
Without lot of introduction, this is a tool to help students get into the mindset needed to thrive in a flipped classroom. These are not “rules” – More like guidelines. Except for #8.
Come prepared. Do the reading and homework in advance and watch the videos.
Prepare to interact, part one. Passivity is the enemy to the type of learning we strive for in class. When you do the home work, interact with the material to develop questions on the areas you need to understand.
Prepare to interact, part two. Bring your questions to class and engage in dialog. Study with a group.
Think about “meta-cognition.” You are training your brain to think like a nurse. This involves a system of logic. You can speed this along by thinking about how you think. Put it on the table.
Talk with more than just the teacher. You can learn a lot from the person next to you.
Stay to the end. If you have already mastered the material, you have an obligation to help your peers. Leaving the dialog is a selfish act.
Stay engaged. “Being present” is more than just being present. Put the smartphone down and nobody will get hurt. Exhibit attending behavior at all times.
Respect those around you. Incivility has no place in this classroom. Examples of incivil behavior can be found in Pearson Volume II page 2650.
Find a way to use nursing therapeutic communication in all that you do. Every peer; the faculty; the patients; hospital personnel; your own family.
Develop a personal “centering practice” and cultivate it. Remember the “First Rule of Knowledge” from the Buddha.
Now that Christmas is over, it will fade out of sight in the rearview mirror as we hit the gas for our destination – 2019. Naturally it starts out as a year full of promise.
Destination – picking up the USA team.
Every good road trip benefits from companions. As in the past, I am willing to bring others with me to experience Acute Care Global Nursing. I am particularly interested to find people to teach PALS and pediatric critical care. The ability to “Code Switch” or learn how, is essential. If this is you, contact me.
Destination – Kathmandu!
CCNEPal will return to Nepal in summer 2019 for about ten weeks, beginning in mid-May – the day after my teaching job here in Florida wraps up the spring semester. I will fly into Kathmandu of course, spend a day or two organizing things, then head off to the Terai.
Destination – Widespread Clinical Competence!
The main question for me is how to maximize the teaching of the course I do so as to reach the widest possible audience. Last year I had the pleasure to re-connect with persons who I taught five or more years ago and I was flattered when they relayed how important that course had been for them, in terms of building confidence and competence in emergency situations. At this point, I have trained about 4,000 nurses and doctors. It’s true that many joined Nepal’s medical “brain drain” – I bet that 300 are now using those skills in Australia. But most are still in Nepal and there has been progress in shifting the mindset.
Since I first started going there specifically to teach critical care skills, there have been many positive developments. The Nepal Society of Critical Care Medicine has gained prominence and taught more short courses – The one titled BASIC has become more accepted. The Critical Care Nurses Association of Nepal was formed and they have helped develop critical care preceptorship models that are now being adopted more widely. The Center for Medical Simulation came into being and they run a fully-certified American Heart Association International Training Center, along with having all the manikins and simulators we take for granted in USA. Many nursing faculty from schools around the country of Nepal have taken the course and they too, will bring new confidence passing the skills to their students. During the 2015 earthquakes, hundreds of nurses and doctors trained by me were able to use their skills to save lives. Also as a direct outcome of my training, many Emergency Rooms and Critical Care Units are now equipped with the communication skills and de-escalation techniques that mitigate the threat of “thrashing.”
Destination – the Terai!
As in the past, most of my efforts are centered in the Terai as opposed to Kathmandu. When I left Nepal in 2018, I was talking with my main partners in Terai about ways to use one of the medical colleges as a more well-defined home base so that nurses and doctors in the region could come there. I need to see if this is still on the agenda. If we can collaborate effectively, we will be able to schedule twelve or fifteen sessions of the course right from the git-go and each one will have the maximum number of enrollees.
To arrange a session of training with CCNEPal in 2019
I will still have availability to go to other regions to teach. A few years back I wrote the terms under which I will deliver a session. Here they are, again.
* * * * * * * * * * * * * * *
How to host a training session with CCNEPal summer 2019
Contact me by sending email to joeniemczura@gmail.com
I will travel to locations outside Kathmandu if the host can do the following:
provide a class space suitable for the program. This needs to be a big space. We move around a lot during this class. It needs: 1) a whiteboard (I do not use PowerPoint) 2) thirty chairs, 3) five patient beds or trolleys for the role play scenarios. 4) air con if possible. The classroom needs to be away from a patient care area. ( we make a lot of noise).
provide a roster of thirty nurses and/or doctors or MBBS students for each session of two, or three days. Nurses take a 3-day sessions and MBBS take the 2-day/ Each participant must attend all sessions of the same class to get the certificate (in other words, the three day class is a three day class – not three one-day classes). arrange for morning chiya and lunch, if there is not a cafeteria.
The sessions are for PCL nurses, B SC nurses, or MBBS. I do not register ANMs in the class. It’s okay if the person is a recent graduate, but the persons need to be working in acute care or intending to work there.
while at a place outside of KTM Valley, the host provides fooding and lodging. I live simply, it can be at a guest house, no need for finest hotel in town. I eat DBT etc so I’m okay with local food. At some locations, they lodge me in a private room on cabin ward. ( they do not need to check my vital signs though!)
My preferred schedule is to teach six days per week, either two three-day sessions (for nurses) or three two-day sessions (for doctors). I travel on Saturday and repeat. In summer 2016 I stayed two weeks in Pokhara, two in Bharatpur, two in Janakpur, and three in Biratnagar before returning to Kathmandu.
I try to make a “circuit” of sessions, not go out-and-back from Kathmandu all the time. It’s more efficient.
I supply the certificates. I keep a minimum amount of photocopy but we need about six pages per person.
My Nepali is poor ( I am ashamed to admit). Strange as it may seem, that is not an insurmountable obstacle if there are some English speakers. I adapt my teaching techniques so as to “Code Switch” in a certain way. If a person has no English, this may not be the class for them.
Destination – home again!
I have loved the past trips to teach in Nepal, but I also love my present teaching job. At the end of the summer, the jalopy pulls into the driveway, we shake the dust out of our clothes, and resume our “normal” lives.
This blog goes a bit dormant when I am back in USA. I returned to my teaching job at an Associate Degree nursing program in Tampa Florida where I carried an ambitious schedule. I was still commuting from Tampa to the Plant City campus, where I taught one section each of the three main courses of the first semester. Here in Tampa I spent the first six Saturdays helping out in the skills lab of our evening/weekend group. I brought two clinical groups to one of the largest most diversified medical centers in the state.
One of my Fall 2018 clinical groups. I think I have had more than a hundred clinical groups in the years I have been teaching.
I was busy.
Ivory Tower
Over Christmas break I am finally able to be back in Ivory Tower mode. Til now, every time I have had a break I go to Nepal, or to the Pine Tree State (Maine) where one of my daughters is fixing up a house with my son-in-law. I was there last Christmas during a cold and dark time, in a partially-heated building, living like somebody “North of the Wall” in Game of Thrones.
View out the glass doors in Maine, December 2017. I was working on my daughter’s house for a couple of weeks. One night about a foot of snow came down. We needed to shovel a path to the barbecue.
This time I decided not to go anywhere, and to simply catch up on things.
For spring semester I will still teach the classroom and skills lab of the groups in Plant City, but cut back to just one clinical group which will be here in Tampa. For three days a week, my commuting time will now be much shorter. This ought to simplify my life. Click here for a short video of me inspecting my student’s work at clinical.
Canvas
Our program uses a computer-based course software system as all colleges do nowadays. Ours is “Canvas.” When it is realizing its potential, Canvas is an amazing online guide, with a grade book, discussion boards, a syllabus, a set of calendars one for each course, and a smartphone app that allows everyone to view assignments and get reminders to keep on track. The problem with Canvas is that it is only as good as the content that is uploaded to it. In the past semesters I usually returned to Tampa just a short time before the upcoming first day of classes, then threw it together in a general way. I uploaded the bare bones of the courses I taught, and I added more as the weeks of the semester ticked by. When you teach the same course for consecutive semesters, you can export the previous content to the new course. In this way my Canvas pages accumulated a volume of content that kept the students mostly happy.
This is the calendar interface for one month Spring Semester 2019. All the ingredients are right there on the list. There are likely to be some students for which the sight will provoke an anxiety attack. We will help them get over it and mobilize their study time.
I began to prepare for Spring 2019 by importing my content, giving myself a nice starting point. After all, the bones of the course are dictated by the overall curriculum and I already know what we will discuss in Week 11 for example. What is new is that I am taking ample time to enhance the content in such a way as to provide the clearest possible directions to the students for them to meet all our target outcomes.
Mea Culpa, Mea Culpa, Mea Maxima Culpa
Last semester we changed from the second edition of our main text to the third, but I did not revise all the reading assignments according to the new pagination. We adopted a new companion workbook but I only assigned things from it for part of the time. These days I am going through lists of reading assignments and double-checking to eliminate or minimize the inaccuracy. Looking at the textbooks myself to make sure I can refer the students to various places they need to go. Maximizing workbook assignments and pro-actively thinking of ways to do in-class exercises to support each one. Also, finding relevant videos to accompany the class sessions.
The Teacher’s “Craft”
This type of planning is what we call the craft of educational design from a classroom management viewpoint. It seems simple an elegant for the student but when you take it apart it has depth that may not be immediately apparent. I am not a fan of detailed work like this but it was overdue. When I assign the students to go to page 2494 and find exemplar 36A, they will find the page number matches the location. I have a library of PowerPoints to accompany the course, and a supply of activities we can do in class as group work.
It will be grand!
Video, Narrated PowerPoint, etc
YouTube is still somewhat new, but it seems as though many people have uploaded bits and pieces of video that amplify or clarify areas of content that we all share. These days there is so much video available, that if I go through the trouble to find it and evaluate it ( “curate it” in the lingo of today’s youth) I can string it together so that there is a reference lecture on video to accompany just about every section. When I add each link I am careful to include the length of the video. When the students access the smartphone app, they will be able to call up a number of pre-recorded files, so they can listen while driving, or also watch the videos anywhere they may go, to fit whatever time is available. The on-line component is so strong that it is approaching the level of an online course. With any luck the classroom portion will take it up a notch.
Guest Faculty
Renowned Faculty with Guest Lecturers from Australia, Kerala India, New York City, and California. I may be the lead teacher in the three courses, but now the virtual course faculty includes about fifty other experts on various other topics, delivering well-researched material with often excellent graphics. It frees up our face-to-face meeting time so we can discuss the material and apply it, instead of transmitting facts and things to memorize.
Do you need an example? this clicking on this video of nurse doing a head-to-toe assessment. We spend weeks teaching the components of this and I always end up modeling how to do it. There needs to be a system but it requires the nurse or nursing student to be interactive. In the video, the nurse hits all the major points. Not only that, but the same people re-did the video with a voice-over play-by-play worthy of Major League Baseball. Sharing this with the students will point the way for them. And yes, this shows a big part of what hospital nurses do all day.
Bicycle etc
I am also taking time to relax, just enjoying my flat. I decided to splurge and get myself some presents – a book I wanted, a small white elephant, a spice rack for the kitchen – that sort of thing. It’s the nice weather season in Florida and I am also trying to ride each day. In about ten days we start the Spring semester. I will be ready!
I’m a Canadian nurse and educator, planning a trip to Nepal in the spring. I have been to Nepal twice before (about 30 years ago) with my husband, we loved the culture and country very much. In 2012 and 2014 I volunteered (the second time with a 4 person teaching team) in Bangladesh at the Grameen Caledonian College of Nursing. We offered some workshops to teachers in their nursing program on moving patients safely, CPR, team teaching, skills (venipuncture, etc) and while there we had an opportunity to visit local hospitals and clinics. Our visit to Nepal would be for about 2 – 3 weeks.
We’ve applied for a small grant to help us come to Nepal to have a similar visit. We’ve been in touch through Nepali friends with the Nursing Dept at Tribhuvan University. We would also like to connect with a school that offers the ANM program.
In Bangladesh we were able to donate some supplies and equipment through our own fundraising (venipucture arm, cpr mannequins, sliding sheets, etc). We would be prepared to do so in Nepal.
I’ve read your articles before and just thought I’d get in touch to see what suggestions you might have.
Thank you, Debbi Templeton
.
.
This made me smile
How could I ignore such an email? I sometimes get these, and it’s always nice to chat, so I gave her my phone number. We had a delightful conversation. Debbi and her colleagues are just the sort of person who can contribute to nursing education in Nepal.
Ms. Templeton has her BSN from McGill University in Montreal and a MSN from the University of British Columbia. McGill is probably the top nursing program in the country of Canada.
She would be joined by three other nursing educators from the Chateauguay Valley Career Education Centre, located in a rural suburb of Montreal, not far from the border with Vermont, USA. (oh, and her husband, who is not a nurse).
Here is a photo showing the group wearing their kurta in B’desh:
Debbi, Kim, Bev, and Daniele
and they toured a tea plantation:
How we can make this work:
Letter
First, for them to get travel funding from the Canadian Government, they need a Nepal host school that would provide them a letter of invitation. As I understand it, such a letter is legally accepted by the Nepal government to allow them to teach nursing while in Nepal.
Previous international travel
This group has volunteered in South Asia in the past, as well as central America. This is not their first trip overseas.
Pokhara? Bharatpur?
Next, they will happily collaborate with Nepali nurse educators while in Nepal. They will start in Kathmandu but they are intrigued by the idea of getting out of Kathmandu Valley.
Contact them:
Debbi Templeton is on FaceBook, send her a friend request and get the dialog going!
Her email address is:
drkbbtempleton@gmail.com.
This kind of exchange is really wonderful when it works. For me, my blog, the CCNEPal FaceBook page, and the YouTube channel are set up to help westerners prepare for such kind of travel.
This is “late” seeing as how I returned to USA six weeks ago. My job in USA – my “real job” keeps me busy.
Locations and hosts
CCNEPal taught 19 sessions in Nepal in summer 2018, and distributed 593 certificates for our flagship 2-day or 3-day course in Critical Care skills.
CCNEPal taught at:
the National Trauma Center (two sessions),
National Burn Center (two sessions), and
Mediciti Hospital (four sessions).
Then two sessions in Janakpur, following up on the visit of two years ago.
After that, four weeks in Bharatpur. CCNEPal taught College of Medical Sciences interns and nurses, also Narayani Samudayik Hospital and the Zonal Hospital.
Back in Kathmandu, the last session of the summer was at CIWEC Clinic.
Special Guest Colleague
I always put out an announcement for other USA critical care nurses who wish to learn about Nepal health care. This summer, Valerie Aikman, RN, BS, joined me for the ten weeks. While I was teaching she was making hospital rounds and applying her experience as a critical care manager alongside the managers of the host institution. I think people really appreciated her expertise in improving the clinical environment for critical care.
Summer 2019
I plan to seek out other nursing educators for summer 2019 as well. We are always asked to provide specific education on pediatric emergencies but I don’t feel like I personally am qualified to teach this; I don’t have the kind of i-depth knowledge of PALS that I do for ACLS.
At some point I will post a more detailed description of what the experience involves.
The doctors of Nepal are leading a nationwide protest by shutting down hospital services except for emergency cases, starting today ( well, strictly speaking, yesterday since they are a day ahead of us on the International Date Line). The government revised the criminal code to establish a criminal penalty for the doctor when a patient dies under their care. The Nepal Medical Association called for this to be suspended until it can be replaced, but the government did not respond to a two-week deadline.
“All Doctors Will Be In jail Due to New Criminal Code”
Writing in Setopati ( A Nepal online publication), Dr Chakra Raj Pandey wrote:
Our attention has been drawn to some provisions related to doctors and health practitioners in the new General Criminal Code that came into effect from first Bhadra, 2075 (August 17, 2018).
Clause 230 (1) and (2) is full of flaws. It seems that people who do not know anything about medical science have proposed the clause. In fact, it can take many individuals lives. There is nothing small or big in medicine. One tablet can cause anaphylaxis or one surgical incision can cut nerve or artery or even cause septicemia.
Medical error has been defined as an unintended act or one that does not achieve its intended outcome, the failure of a planned action to be completed as intended (an error of execution), the use of a wrong plan to achieve an aim (an error of planning), or a deviation from the process of care that may or may not cause harm to the patient. Heart ailments cause 611 thousand, cancer 585 thousand and medical errors 251 thousand deaths, according to statistics from US Hospitals for 2013.
Looking at clause 230 (3) and (4), any of us can be in prison from three years to whole life.
Hippocratic Oath prohibits all of us from treating any patient with wrong intention. If we do so, we are not physicians. In that situation, our license has to be confiscated by the council or other regulatory bodies. …..
Clause 231 (2) a and b treat malicious treatment by physicians like murders. They state that no physician will treat maliciously, and the physician’s license will be confiscated if there is any concern and complaint about malicious treatment. I have never heard and read about any physician treating maliciously in my life. How can a patient go to a physician who is treating maliciously?
Clause 232 talks about medical negligence. Is it medical error or is it a different thing? If we talk about medical error as medical negligence, there will be no space left in the country’s prisons and there will be no doctors left in the hospitals.
He continues:
So, this law has been put forward without enough homework and no stakeholder was invited in the discussion process. It is still not too late to correct it. I am sure with the able leadership of Prime Minister KP Sharma Oli, this problem can be corrected once and for all.
The discussion, in my view, has to be focused on how to produce able doctors, how to provide life-long education, how to participate in maintenance of certification, how to do clinical and basic science research, how to make better hospitals where doctors can perform best surgeries, treat patients in the best possible way, and how to build safe institution.
It seems our focus has deviated from the main goal. Let physicians and allied specialties come together to show the correct path and solidarity.
Background to the issue
The problem is, Nepal is a Low Income Country with tremendous geographical challenges and an underfunded health system. There are many “excess deaths” in all regions of the country, an “excess death” being defined as one which might not have happened if the best possible medical care had been applied. A number of these inadvertent bad outcomes garner nationwide publicity. Most notably, for example, if a woman dies in childbirth it is not unusual for the relatives to assault the doctor, vandalize the hospital and demand compensation. The link will take the reader to a partial list of well-publicized incidents maintained by CCNEPal.
Deja Vu, All Over Again
In September 2017, the NMA strongly protested a similar proposal, one that would have also criminalized the practice of medicine. The government ministers have not gotten the message it seems. At that time an editorial in SwasthyaKabar wrote:
Doctors all over Nepal are now hesitant to take any risks by managing complicated cases on their own, thus leading to many unnecessary referrals to higher centers. This is what they call “defensive medicine.” Many hospitals are not managing serious cases because of the fear of repercussions if anything goes wrong. They are putting their safety first and being defensive, especially in those areas where they are practicing in small groups without much supervision and guidance. This will lead to a significant increase in the number of cases burdening the public health care system, thereby further decreasing quality and increasing the cost of clinical care. Patients will be directly affected if this continues. The patients from the most vulnerable and marginalized population will be the ones most dramatically affected, given that they do not have any alternative, and cannot afford to pay high out of pocket expenditures to go to private clinics. Health care will not be equitable and affordable to all, by any means.
Root Cause analysis
The custom in Nepal is to simply blame the doctor. In USA we would “drill down” to examine the safety systems in place to pro-actively identify hazards, but nobody seems to have applied this to Nepal before adopting the new law. For example, determining if the hospital owned the right emergency equipment and whether it was in good repair, or perhaps whether the staff was properly trained. Questions such as whether the patient intentionally delayed going to the hospital or did not enroll in prenatal care. One international NGO that runs a hospital in Nepal did publish one of their own such analyses recently, and it illustrates the points I am making.
Transfusions as an illustration
Nepal does not have a consistent blood banking system, but does have a population of citizens with AB+ blood, a situation that becomes dire when the person who needs it is a postpartum woman in hemorrhage. (Not the only problem with Nepal’s system for transfusion.) The way the new law is written, any doctor unable to obtain AB+ blood for such a patient can go to jail. If this is allowed to let stand, who in their right mind will risk agreeing to deliver the baby of any woman at risk?
Thrashing of doctors and vandalizing hospitals
This is already an issue in Nepal, and in fact it is a problem in all South Asia, as has been documented in this very blog you are now reading. Regardless of the circumstances of death, it is a widely known cultural practice to blame the doctor and attempt harm. In the recent past, India and other countries have considered a #JailWithoutBail penalty for any patient party that reacts to bad medical news with violence, modeed after a newla in Queensland, Australia. This new law in Nepal achieves the opposite effect, and increases the likelihood that doctors will get thrashed and the perpetrators will be immune from prosecution.
A prior protest by doctors in India to raise awareness of the risk of being thrashed by angry relatives of a patient. The risk of thrashing has nothing to do with the quality of care being delivered.
There is no central registry of inadvertent deaths
The government has no data of which I am aware, which is why I started the tally of cases that received newspaper coverage. There are many equally serious cases that do not receive coverage because they lack the sensational element. In my travels around Nepal teaching critical care skills to doctors and nurses, I listen to many anecdotal stories of systems failures.
Government Hospitals
It is crystal clear that any doctor working in an underfunded hospital can easily become a scapegoat. The biggest most underfunded hospitals in Nepal are the District Hospitals and Regional Hospitals. Even more so in rural areas. Why would any young doctor take the risk and work in a rural government hospital?
Protest in Kathmandu
Here in Nepali language is a video of a protest march.
These are not the kind of people you ordinarily expect to be out marching.
Other background info
More information as to other new and controversial clauses in the newly revised law are listed here.
Summary
This preset proposal needs to be withdrawn and all stakeholders need to have input.
This blog is directed to my videshi readers. I am pointing out the need for videshis to adapt to the culture of Nepal. I invite comments but I will only publish if they are respectful.
Give yourself time to click on every blue link.
Update: I am told by multiple persons that “code switching” is what I am talking about. I confess my ignorance in not knowing what every else knew! There are ample links about code switching, and anthropologists have popularized this term. I will write an entire blog on code switching in my context, once I digest them all. Global Health Nurses! Learn to code switch! Here is a ten-minute video from a linguist.
I am fortunate to enjoy a good reputation for my sessions. Here is a Nepali-language sample of feedback from a person who took my training:
Travel Back in Time
Seven years ago I once wrote a blog titled “Twelve Steps to Prepare for Global Health Nursing” which made the case for easy ways to learn about the culture of whichever country a nurse might think of going. I re-read it recently and it withstood the test of time. There is one area to add, though, specifically on the topic of teaching nursing in an English-speaking low income country.
Imagine yourself in a classroom with this guy as the teacher:
Now imagine that these guys are your students and this is the level of English they speak. I have taught many of my sessions outside KTM Valley where this is the level of English possessed by much of the class.
Now imagine this is the lecture you are trying to deliver to those guys:
The American guy in the video obviously knows his stuff. The speaker is knowledgeable, speaks clearly, makes his points including nuances. Tell me honestly, will they get it?
The answer is obvious. 1) he talks too fast 2) he uses too many big words 3) he uses complex grammar. 4) not enough time for students to write notes 5) complicated graphics. 5) no pauses for people to process.
He is a terrific lecturer for America audiences but he would be frustrated in Nepal.
There are many Nepali people with excellent English, don’t get me wrong:
Pronunciation
English is not pronounced in Nepal the way you think it is. Here is some info about the way words are sounded out:
“The language of instruction is English,” I have been reminded in about two dozen locales of Nepal, by various and sundry. This is said of Nepal (which was never conquered or colonized), but it also applies to such places as India, Nigeria, Jamaica, Guyana, Singapore and other former colonies of Britain.
Um, no. It is not. To truly become successful you must understand the idea of hybrid English, also known as “Pidgin.”
ESL
The language of instruction in Nepal is English as a Second Language (“ESL“), not English. There are lots of Americans ( and Brits and Aussies) who don’t know the difference. ESL implies that the student’s grasp of English has very specific limits. In USA these days any given nursing school will always have a subgroup of ESL students, and they often need coaching as to how to grasp “medicalese” – (when you get down to it, most medical professionals don’t speak English either!).
Because of the Medicalese issue, I learned long ago in USA to treat my entire classroom of beginner nursing students as if I was teaching them a foreign language. Think of all the abbreviations a practicing nurse or doctor will use in daily work. I am very proud to say that my current employer ( a community college) devotes resources to the success of these students.
Back to Nepal and “Foreign Lands”
The ideal of course, is for every American volunteer abroad to speak and teach in the local language.
When learning the local language is not possible, it is very important to adapt your own language so that it mirrors the English the students speak. Assess the level of language skill of your listeners very carefully, and reserve your most erudite English only for those at the top tier of English proficiency. Switch your style to fit the audience.
There are people who get it, and others who keep the same speaking style they use in USA, telling themselves something like “I’ll help people more if I model my mastery of the language and elevate the English comprehension of the listeners.”
Nope. That lasts about a minute. The audience will be lost and confused. They will politely listen because after all, you are a foreigner and you have come such a long way. But if somebody asked them what you just said, they are unable to describe it.
International Conference in Kathmandu
I saw this in the ballroom of Kathmandu’s Hyatt Regency a few years back when a distinguished cardiac surgeon from USA was speaking to two hundred people about developments in mitral valve surgery. I thought it was interesting. But, most Nepalis in my vicinity sat politely, looking at FaceBook on their mobile. The conference was funded by the University in USA that sent the surgeon; they subsidized the conference registration fee for most of the listeners; but the points sailed right over the heads of the people in the chairs.
The Nepalis themselves put on better conferences organized by Nepalis for their own colleagues.
International Conference on USA East Coast
A few years back I also attended an event for Global Health Nursing in which the keynote speaker recycled a scholarly paper to present to an audience that included many academics from USA interested in Global Health, but also many nurses from outside USA. My assessment? She too, failed to read the audience. The nurses from Haiti and Africa in attendance did not quite get it. I wonder, when we send doctorally-prepared nurses abroad, do they use this level of language? If so, are they really imparting anything of value?
Does Incrementally Erudite Scholarly Presentation lead to cognitive comprehension?
There is need in global health nursing to use plain language for the benefit of all concerned.
In an ESL classroom, the focus is on the learner and what they comprehend, not on the teacher. It’s a spectrum I suppose, but I am proposing that we slide the marker to the right a bit…… tilt it more toward the learner.
Book culture in Nepal
Back to Nepal. the day-to-day culture here is not one that reads a lot of books. In nursing school here, people don’t study an English-language textbook by themselves. Five students gather round. The person with the best English reads it out loud, then they discuss what they just heard, in Nepali.
Here is a video I found from India, it’s a YouTube summary of a scholarly paper on this as applied in India ( a neighboring country whose language has similar origins to that of Nepal). This makes me want to read the original article! The video is 37 minute long, but it dives in to the subtleties of how English is spoken in India and ways you can use “code talk.” The examples this person gives are in Hindi, similar in many ways to Nepali (um, Nepali is much more musical and beautiful if you ask me).
This teacher has other videos.
Singlish
Here is a video about the amalgam of Language in Singapore (Um, Not Safe for Work!) . There are surprising parallels to the way English is spoken by many in Nepal, and I know one Nepali nurse whose father was deployed with Gurkhas to Singapore, so her English is almost exactly like that of this narrator:
I have always loved Pidgin languages. I lived in Maine a long time, famous for a peculiar accent, and a vocabulary that mixes archaic words from Elizabethan England into English. I can easily speak like a native Mainer and certainly my two daughters are fluent. I also lived in Hawaii, where there is an even more distinct pidgin (you need to click on that link!) that incorporates many phrases and grammar of Hawaiian language as well as Filipino, Japanese, and Chinese. I am unable to imitate this at all, due to the inflection and musicality. I totally loved and respected the way this is a living language and the politics of it are fascinating to me. The musicality of an Asian language, and the grammatical differences tend to accentuate the difficulty in hearing what is being said.
Jamaica?
Listen to this one.If you can’t somehow get it, you need to tune your ear:
Some of the points about preparation in my original article reinforce this, such as spending time with the local Nepalis in USA before you depart for Kathmandu, but I think this ESL issue needs emphasis so that you have a clear goal when you are speaking with your American-based Nepali friends and preparing yourself for cultural awareness. It’s about more than just food and prayer flags.
Future blog on this subject?
there are many things I consciously do in my classroom to address this specific challenge, some I have been doing so long I realize I take them for granted. Here is one specific example:
the actual ten steps of defibrillation are the same whether you learn them in English or in Nepali. I always start each of my own classes by telling the group “you can be expert at resuscitation even if you speak no English whatsoever”
Bullet Points?
In a future blog I will give a list of bullet points for things to focus on when preparing for your own global health teaching experience. Until then, looking forward to your feedback.
In Summary
Add training and study of ESL principles, and even some guided practice, to your to-do list before going to teach nursing outside the boundaries of USA. Even if it is to a country where many speak English, you still need to study the language. You will be glad you did!
So the last teaching session for 2018 finished yesterday.
Final tally:
sessions: 19
total certificates: 583. These are easy to quantify.
Nursing consultations: many. Not so easy to quantify, perhaps priceless! Valerie Aikman, RN, BSN is an experienced and qualified nursing administrator and critical care manager who collaborated with administrators at every host agency. I expect that she will share her perspective in future guest blogs on this site. She brought a unique skill set to Nepal.
Valerie Aikman, R,N, B. S was my colleague this summer. Here she is with Anupama Karnajeet, RN, B Sc who first took my course five years back. Ms. Karnajeet is a critical care specialist in her own right. Her assistance was invaluable.
Last session, back in Kathmandu
We taught 24 nurses from CIWEC hospital. This one was arranged through a former CCNEPal participant now working there, Anupama Karnajeet. CIWEC is located in Lazimpat, convenient to the big hotels and near the former royal palace. I usually focus on hospitals in other parts of Kathmandu.
Calling Doctor Rajasthani
This training does not use PowerPoint. We do not own expensive manikins. We do not have long periods of lecture. we are hands-on and practical.
Just a small number of costume items makes training more fun. Doctor Rajasthani is a recurring character in the drama…..
CCNEPal tends to work in Terai these days with only short periods in Kathmandu. They were having construction at the hospital so the venue was the meeting hall of the Himalayan Rescue Association nearby.
Himalayan Rescue Association has a nice space for class size of thirty.
CIWEC
CIWEC Hospital has an unusual history. It was originally a Canadian project,since 1982. They cater to travel medicine, about 80% of their admissions are foreign tourists. They are busiest during trekking season, spring and fall. Here is a 15 minute YouTube video (Nepali with English subtitles). The two doctors in the video also speak excellent English for those who care.
Everest route. If you trek to Everest Base Camp and develop frostbite or HAPE, you will most likely be evacuated to CIWEC. The Tourist Association of Nepal has a system to help injured travelers.
They are famous for treatment of diarrhea, a tourist plague; CIWEC participates in research on this illness.
CIWEC gets patients with frostbite, a problem among climbers. Among the expatriate community of Kathmandu, they are the most highly recommended of any Nepali hospital.
Poster in the OPD area. Nobody is downplaying the seriousness of diarrhea, but it’s nice to retain perspective.
Th physical plant is the closest thing to a western hospital, in the country. The mineral content of water here seems to easily corrode plumbing, for example, making faucets difficult to operate. CIWEC does not have this problem. The hospital was remarkably clean and reminded me of my own doctor’s office back in Tampa.
The rooms were nice.
Most of the inpatient rooms at CIWEC are single-occupancy but some are double. Bright and airy. The closest to a USA hospital room of any place.
Obviously I just spent three days with the nursing staff. They all were multilingual and spoke good English, as advertised. Many studied or worked overseas.
The course ” Assistants”for this batch. One of the classroom management techniques I use is to delegate running the megacode drills to people who speak better Nepali than I do!
brushing up on ecg rhythms. I teach the six step method, the international standard. the class was attentive and sked good questions.
Many previously took either BLS or ACLS and worked in critical care in other hospitals prior to joining CIWEC. The hospital is able to recruit and retain the best.
part of the three-bed ICU.
Emergency Room at CIWEC
The ER consists of two well-equipped single-stretcher rooms.
each ER room has’s own ambulance door and an inner door. They have a “minor Operating Theater” adjacent to the ER as well as a larger O.T upstairs. They can do endoscopy.
I wrote relatively little this summer on this blog, I was busy teaching. I expect to backtrack over the fall and fill in the gaps. This will include ideas about summer 2019.
July 22 update the trip back to Kathmandu was uneventful. The temp here is is in the 80s (f) as opposed to 100 (f) and it is amazingly quiet at night when you don’t run the air con. For some reason my spellcheck keeps correcting it to zircon.
We are now in the “Shalom Annex 3” since the regular Shalom is full-up with medical students from Newfoundland. it is near Ekantakuna, a pleasant little chowk. We got groceries and put them on the pantry shelves.
We were chatting on the back porch, when we heard a noise in the kitchen. It was a monkey that snuck in through the window. He had opened the fridge and strewn about some noodles. We scared him away. the neighbors came, so did the other boarders. We learn that this guy has been patrolling the area.
Alas, no photos of the kitchen scene.
We named our neighbor “Curious George” of course.
July 22nd, 23rd and 24th CIWEC Clinic in Kathmandu. The actual training hall will be at Himalayan Rescue Association in Lazimpat.
July 25th, to Aug 2nd – open dates. we will meet with supporters and friends in Kathmandu… time to “stop and smell the incense” and there are many persons we wish to meet with before we leave so as to set things up for next year.
August 2nd – rendezvous with TIA for flights to USA.
we now have about two weeks remaining on this trip. We have taught seventeen sessions and given 489 certificates. We will give about a hundred more if all goes to plan.
Valerie Aikman,RN, BSN has been a wonderful addition to the CCNEPal team, offering a level of consultation on nursing issues I was not able to do in the past. I will write more about her in the future. She will most likely write some guest blogs.
Calendar:
July 15th, 16th, 17th Narayani Samadayik, Bharatpur. We will work with a very longtime colleague, Dr. Kalyan Sapkota. This will be a three-day session and include nurses from the District Hospital here.
July 18th, 19th and 20th – one last 3-day session at College of Medical Sciences. for nurses. We have truly enjoyed our collaboration with College of Medical Sciences, and we are discussing how best to work together in future.
July 21st – return by airplane back to Kathmandu Valley. Since monsoon there are more landslides on the Mugling-Narayaghat highway. Since my bus accident a few years back I plan the travel so as to take the fewest bus trips possible. Therefore, a plane ticket. We did take one bus from Janakpur to Chitwan.
July 22nd, 23rd and 24th CIWEC Clinic in Kathmandu. The actual training hall will be at Himalayan Rescue Association in Lazimpat.
July 25th, to Aug 2nd – open dates. we will meet with supporters and friends in Kathmandu… time to “stop and smell the incense” and there are many persons we wish to meet with before we leave so as to set things up for next year.
August 2nd – rendezvous with TIA for flights to USA.
This is the updated itinerary for CCNEPal as of June 9 2018.
We have taught six sessions since arrival, with 179 certificates given. We will do two more three-day sessions this week in Kathmandu, at Mediciti Hospital. Mediciti has been a wonderful host and I love the staff there.
At this rate we will train about 600 nurses and doctors in Nepal this year. We already trained 3,200 in past visits.
“This is not like other training”
I get similar feedback from every group. “Nobody told us what to expect, so I thought it would be one more lecture day by a videshi using all PowerPoint and many handouts. It turns out to be very practical and hands-on.”
Anybody can teach the drugs, how to do CPR, and read an ecg.
Not everybody can teach confidence, teamwork, poise and how to think under pressure.
I lie to think we are transforming the way people look at their role in critical care, and soon I will expand this idea in another bog. Not today, though.
Next Stop
We travel to Terai June 16th, by plane to Janakpur.
June 17th,18th and 19th, then 20th, 21st and 22nd. – two 3-day sessions at Janakpur. This is also a return visit. In 2016 we worked to develop ICU staff there. I am pleased to report that JHCRC is now offering a full range of critical care services, such as thrombolysis. We expect to focus on schools of nursing there, to ensure the supply of nurses. This will be Valerie’s introduction to the Terai.
I asked to take a photo and the shopkeeper got a new vat of yogurt out of the fridge. the yogurt here is every bit as good as the fabled yogurt of Bhaktapur!
Travel day June 23rd. long distance bus from Janakpur to Chitwan.
June 24, 25 & 26th – College of Medical Sciences (COMS), Bharatpur. Nursing 3rd years. Also known as “Purano.” This first session will be for nursing students. COMS is a location I visit since 2011. Because it is a major teaching facility, people trained here disperse throughout the Terai region.
June 27th, 28th and 29th – College of Medical Sciences (COMS) a second batch of nursing students.
The College of Medical Sciences Teaching Hospital in Bharatpur operates one of the busiest Emergency Rooms in Nepal. They first hosted me in 2011.
July 1st,2nd, 3rd COMS – a batch of staff nurses.
CMS Nursing College in Bharatpur enrolled their thirdyears in the CCNEPal 3-day class. They were really good.
July 4th, 5th, July 8th & 9th, July 10th & 11th – three 2-day sessions for Medical Officers and interns at COMS.
July 12th, 13th and 14th – Maybe time to go to Chitwan National Park so Valerie can ride an elephant and feed a tiger. My personal favorite in that location is the river trip in a dugout canoe to observe wildlife, mainly birds.
July 15th, 16th, 17th Narayani Samaiyudak, Bharatpur.
18th, 19th and 20th? possibly another session in Bharatpur, who knows!
July 22nd through 27th – this is the only remaining week to be booked with teaching or consulting. We can do two three-day sessions (for nurses) or three 2-day sessions(for MBBS). We have passed emails with various hospitals in Pokhara and western Terai but nothing is confirmed. If any body reading this wishes to host a session or two, please contact me at joeniemczura@gmail.com
The first session for this year’s series of training programs in Nepal was held at National Trauma Center, part of Bir Hospital, for a group of BN nursing students. One member of the class had previously taken the course and asked if I was still doing the anatomy lab.
These days? well, no, I haven’t been including it.
Why not?
There was no good answer, so – we enlisted various class members to go to their local fresh shop and find “en bloc heart and lung assemblies” – and we had an educational time that revealed many secrets of the heart.
We are now at a large Kathmandu hospital where we are training four batches of nurses with thirty people in each. We are including the lab in all four sessions of the course. The use of this material of to advance scientific knowledge, and the goats would have been harvested anyway. In fact, the lungs would have been fed to neighbor dogs. There is a nearby fresh shop that supplies five each time, one for each group of six students. Enough to allow each student to get a close look.
We make a systematic tour of elements of the heart, lungs and trachea, finding such things as the pericardial sac, the valves and the coronary arteries. No matter how well the teacher can draw, there is no substitute for seeing the actual structure. Each nurse who participated will now make better physical assessments of their human patients because of the knowledge they gained.
Here is an example from YouTube that shows one way to do the dissection. https://youtu.be/XH4K4b0N_Yw I think it has the info, but I don’t lead my own labs that way – she’s is a bit passive, doing all the handling herself. It’s more fun to make the students handle it themselves and discover it for themselves.
Not wasting anything
One thing to point out: when we are finished I end up with about eight pounds of organ meat. I don’t simply throw it in the trash. I take it home and recycle it. Each set of heart & lung gets cut into small pieces. I bring it up to the roof of the Guest House for the crows to enjoy.
I do not waste the flesh or put it in landfill. As many as three dozen crows swoop in to take morsels back to the nest for their young. There is one day per year in which crows are venerated on the Hind calendar. This batch of crows is getting food every day for two weeks.
The crows get excited when they see me climb the spiral stairs to the top patio.
At Bir Hospital school of nursing, the B Sc program is for nurses who completed PCL then have worked for two years. The focus of education there is to improve medical-surgical nursing and they are keenly interested in critical care. I was there last year and the students were excellent. The “five assistants” are shown, wearing the distinctive uniform sari of Bir.
We arrive May 17th (Joe) and 19th (Valerie) and run around like crazy getting supplies and things organized for a couple of days. Wish us luck!
The schedule is falling into place
May 20th,21st and 22nd – Bir Hospital B Sc students. These nurses have completed their PCL nursing and are going for the B.SC. degree. Bir is government-run. It is the main teaching hospital for NAMS, the National Academy of Medical Sciences, and serves as a free-of-charge resource for people from all over Nepal. Located right on the edge of Old Kathmandu. This is a return engagement for us.
May 23rd, 23th and 25th Bir Hospital Trauma Center staff nurses.
May 26th holiday and recuperation
May 27th, 28th and 29th – National Burn Center staff nurses, Kirtipur
The “HDU” at Kirtipur is the most active critical car unit for burn victims in Nepal. This will be our second trip to teach there.
May 30th and 31st National Burn Center Kirtipur, interns and Medical Officers (2-day)
June 1st and 2nd holiday for two days – r & r
June 3rd, 4th & 5th – Meditici 3-day #1 session. This is a new facility just outside the Ring Road in Lalitpur.
June 6th, 7th and 8th – Mediciti 3-day, #2 session.
June 9th – travel day. From Kathmandu to Janakpur. This begins the Road Trip through Terai. Most likely we will fly there. My first trip in 2016 was memorable and epic.
June 10th,11th and 12th, then 13th, 14th and 15th. – two 3-day sessions at Janakpur. This is also a return visit. In 2016 we worked to develop ICU staff there. I am pleased to report they are offering a full range of critical care services, such as thrombolysis. We expect to focus on schools of nursing there, and we have yet to determine whether we stay an additional week. It depends on the demand for training and also whether we will add a PALS course, etc. specific breakdown TBD ( combination of 2-day and 3-day sessions)
I asked to take a photo and the shopkeeper got a new vat of yogurt out of the fridge. the yogurt here is every bit as good as the fabled yogurt of Bhaktapur!
Travel day June 23rd. long distance bus from Janakpur to Chitwan.
June 24, 25 & 26th – College of Medical Sciences (COMS), Bharatpur. Nursing 3rd years. Also known as “Purano.” This first session will be for nursing students. COMS is a location I visit since 2011. Because it is a major teaching facility, people i train here disperse throughout the Terai region.
June 27th, 28th and 29th – College of Medical Sciences (COMS) a second batch of nursing students.
The College of Medical Sciences Teaching Hospital in Bharatpur operates one of the busiest Emergency Rooms in Nepal. They first hosted me in 2011.
July 1st,2nd, 3rd COMS – a batch of staff nurses.
CMS Nursing College in Bharatpur enrolled their thirdyears in the CCNEPal 3-day class. They were really good.
July 4th, 5th, July 8th & 9th, July 10th & 11th – three 2-day sessions for Medical Officers and interns at COMS.
July 12th, 13th and 14th – Maybe time to go to Chitwan National Park so Valerie can ride an elephant and feed a tiger. My personal favorite in that location is the river trip in a dugout canoe to observe wildlife, mainly birds.
July 15th, 16th, 17th Narayani Samaiyudak, Bharatpur.
July 18th,19th 20th open, any session needs to be in Bharatpur.
(my photo) Rush hour in Sauraha, next to Chitwan National Park. This is what the tourists see. Most cities do not actually have these.
July 22nd, 23rd, 24th possible Danghadi. tentative, CCNEPal has never been further west than BTWL, it’s about time don’t you think?
July 25th, 26th, 27th possible Dangadhi at Zonal Hospital.
The “standar5d class size” is thirty. Five are asked to be “assistants” ans then five groups of five each. So, we need five sets of the flash cards! They are colorcoded. Each assistant gets a laminated list of the possible scenarios we will eventually be doing……. this system is impervious to loadshedding.
Subsequent dates and locations tentative, will be announced as they are booked.
July 28th, travel day. We will disappear from one location and re-appear as if by magic, hundreds of miles away. Here is a short video that explains how this is done:
July 29th, 30th, 31st – one last session in Kathmandu. Historically, CCNEPal has always offered a few first-come-first-served sessions in Kathmandu, and we have been reminded that this year’s schedule has not allowed room for such trainings.
Pediatric Life Support course: we have yet to schedule these sessions, stay tuned.
Nepal is a low income country and the profile of illnesses are not quite what you would see in USA. Read my first book, The Hospital at the End of the World, to learn more.
Summer break. School in USA goes for one more week. Then in two weeks, CCNEPal gets on the plane for Nepal again, teaching critical care skills for summer 2018.
What does CCNEPal do, exactly?
This has been answered on the blog you are reading, right now. Since 2011 I wrote more than 262 entries here. We do a 3-day course for nurses and 2-day course for MBBS docs. I write less when I am in USA and more when I am in Nepal. I have taught 110 sessions of this since 2011, awarding 3,200 certificates. I can easily supply a list of references from Nepali hospital administrators, doctors and matrons who have hosted me. There is also a FaceBook page that supplies plenty of photographic proof as to where I have been and what I have done.
You can also check out my YouTube channel, here is an old video that shows my teaching it’s 24 minutes but still a good representation of the spirit. https://youtu.be/FZjqfOdWRb8
here is a shorter video that shows the class members practicing megacode. it has a narrative that shows how we divide into groups that get the entire class involved: https://youtu.be/HCQmdtmmKVo
In ten words or less, I teach a highly modified version of a ACLS class over the course of three days. We start with CPR but quickly go to team dynamics, how to conduct yoursel fduring an emergency, ecg, defibrillation, and the ACLS protocols. On the final day we also address issues of situational awareness to employ to prevent and mitigate “thrashing” when tension is high.
here is a blog entry that describes how we teach situational awareness using role play: https://wp.me/p1pDBL-Bb
New Team Member
This year I am pleased to announce that Ms. Valerie Aikman, RN, BSN will be joining me. Ms Aikman has a background in critical care management. She will add some unique skills to the project. In USA she works for a company that consults with hospitals regarding critical care, and she works as an “interim manager.” Typically, she goes to any given location for two or three months at time and runs the ICU when the hospital is looking for a permanent ICU manager. Not only does she love to problem-solve and consultate (is that an actual word?) but she is good at it. She has always wanted to travel in Nepal and see what hospitals are like. She has a background in Er and Trauma ICU; I often get asked if I teach a mass casualty triage course and now? we can! She is a wonderful addition to our team.
Schedule of courses
We will be teaching two 3-day sessions at Bir Hospital starting May 20th, one for the B Sc students and one for staff nurses.
then a 3-day (nurses) and a 2-day ( doctors) at the National Burn Center in Kirtipur
then 3-day courses at Mediciti Hospital in Lalitpur. We have confirmed one week, we may add a second week.
After that we will go to Terai, where will teach at Narayani Samaiyudak, College of Medical Sciences, and Janaki Health Care and Research Center in Janakpur ( two weeks).
Usually we offer some first-come-first-serve open to all comers sessions. We will plan to return to Kathmandu and announce some of these in late July.
CCNEPal is (usually) a one-person circus of teaching and we never know whether any given trip to Nepal will be the last one. I have been saying this since 2007, the first year I visited Nepal, that “I don’t think i will ever do that again” – and yet, I do.
Nepal is a bigger country than you think
I am a volunteer, and I always am amused when I meet some other medical person (usually a young MD) and they tell me “Oh, soon they won’t need your training any more; I’m here in Nepal and I am training them how to do critical care. ”
Yes, more than one person has said something like that to me. So, I ask for more detail. Then they say, “I’m here for two weeks and I will work with a dozen people.”
Nepal has 30,000,000 people, 22 medical colleges, hundreds of nursing colleges, and many cities outside of Kathmandu Valley. There are seven medical colleges in just the Kathmandu Valley, and a government health bureaucracy as well.
So, more training is needed to ramp things up. A lot more. Um, I trained 3,200 people in many regions of Nepal over 110 sessions during a ten year period. And we are still getting up to speed. I am happy to say that more Nepalis are stepping up and teaching it themselves, which is the way it should be.
To get ready this year I spent $$$ buying teaching materials for ACLS and PALS.
I always teach as much of the latest protocols as I can, though the American curriculum needs to be adapted to reflect things like the availability of drugs and equipment. I get the protocols from the American Heart Association and this year I got all the bells and whistles – the complete “Instructor Package” including books DVDs and posters.
I also bought the stuff to present the latest Pediatric Life Support standards and protocols.
I have been updating some of the key handouts from my “usual class” so they make it easier to run each course.
Schedule
I will arrive in Kathmandu the 17th of May and begin the first session the 20th, at a major school of nursing in Kathmandu, one where the students come from all regions of Nepal and will return home after their degree. I will be teaching in Kathmandu for about three weeks, during which time we will award about 200 certificates.
After that I get on the bus to Bharatpur, where I will spend two weeks. I am not sure what to expect on the Mugling-Narayangarh road!
the main road from Kathmandu to the outside world goes through a spectacular river canyon and has been under reconstruction since the Dawn of Time. Lots of twists and turns. I try to minimize trips on this road.
I will spend a week teaching in Janakpur also while in Terai. If you wish to host my training, read this previous blog entry on what is needed. This requires a large classroom and at least 30 learners.
Colleague with a Secret Identity?
Nurses never bring attention to themselves. My colleague is carrying on in the finest tradition of selfless secret identity.
A person with extensive experience managing ICUs in USA will be with me, and I will do a blog introducing her soon. She is a USA RN with many years of experience who wishes to share her expertise with her Nepali peers. For now she will be a “mystery person” – isn’t it cool to travel with somebody who has their very own secret identity? Here is the first clue as to who, exactly, she may be.
Okay, so I use this blog to keep a running track of “thrashing incidents” in Nepal. I also list incidents in India since this problem is worse there. Today’s news was about the actual death of a resident doctor in India.
PUNE: A resident doctor was assaulted with a scalpel and a few paramedics were roughed up by relatives of 26 -year-old man after he suddenly died following a cardiac arrest at D Y Patil Medical College and Hospital in Pimpri late on Friday evening.
The resident doctor suffered a deep cut on his face and some blunt injuries in the assault. The hospital management on Saturday filed a complaint with the Pimpri police.
The doctors demanded strict implementation of the Medicare Act, 2010. It protects them from physical assaults and intimidation by patients’ relatives. These acts are non-bailable offences under the act.
A doctor of the hospital said, “After we broke the news of patient’s demise, the relatives burst into rage and barged into the ICU (intensive care unit). One of them took a scalpel and slashed it on a resident doctor’s face claiming negligence. Others joined him.”
Another resident doctor said, “A local politician claiming to be a policeman hoodwinked the security and entered the ICU, where quite a few critical patients were undergoing treatment. He arrived with some supporters within 10 minutes of the event.”
After entering the ICU, they proceeded to assault the men and women doctorsl. “Fearing for their life, these doctors are wondering if they should even go to the police,” the doctor said, requesting anonymity.
The securitymen of the hospital failed to prove their effectiveness during the assault. “The bouncers and security guards employed by the hospital stood back and did nothing. They have been identified and would be dismissed,” said another doctor.
There was some communication gap between the hospital’s senior and middle management. “The middle management did not inform seniors about the scenario. They were afraid of being found out for hiring a bad security agency,” said another doctor.
The hospital’s dean, Jitendra Bhawalkar, said, “We always stand by the side of our resident doctors and ensure that their protection is never compromised. We have filed an FIR with the police in this regard.”
News reports included a photo of the injured doctor, showing the injury with the scalpel. It was very graphic. Originally, I decided not to post it here, which turns out to be a good thing since the graphic photo was from a different person altogether! Also, the viral meme on the internet shouted the news that the doctor had in fact died – this needs to be verified.
If you are new to this blog, please read previous entries on the subject of “situational awareness” and thrashing of doctors. CCNEPal was originally started to provide better training of nurses and doctors in Nepal in the area of resuscitation after cardiac arrest. Soon after starting in 2011, we recognized the idea that the potential for being thrashed if things don’t go right was a major barrier in success. So, we teach about ways to identify a bad situation in advance and deal with it. We expect to be back in Nepal in summer 2018 to train more personnel and raise awareness of this issue impacting medical care.
This will be brief. I haven’t added to this blog in some time, not since reporting on one of the most recent thrashing incidents. This blog provides commentary on issues affecting nursing and especially critical care nursing, in the country of Nepal.
I hope to return to Nepal this summer, as I have done since 2007. Since 2011 I specifically focus on teaching critical care skills to nurses and doctors there. Every time I return I think about how whichever trip I just completed might be the last time. And yet, I get another ticket.
This time is similar. I have ideas as to how I can contribute but never is ever firm until I commit by buying the ticket.
Want to host CCNEPal?
I want to hear from people interested in hosting the training. I will spend part of the time in Terai and a bit of time in Kathmandu Valley. In 2017 I needed to cut the time short and not fulfill promises I made to teach at certain places. I want to follow through despite the problems. I am not destined to only teach at certain places but not others….. the overall goal is to advance the practice of critical care in Nepal. How can we work together to accomplish this?
Family
One of my daughters tells me she may visit Nepal this time and if she does I will take time to be a tourist and show her around. My other daughter has been lobbying heavily for me to join her in Maine as she works on the old farmhouse she bought. I love spending time with these two young women.
Browse
Feel free to browse the 262 previous entries on this blog. I love getting feedback!
at some point, riot police were called. The typical weapon of police is the lathi, a four-foot stick.
This was first reported in OnlineKhabar, Nepali language. Rebublika published it after a day.
GULMI, Dec 21: A patient admitted to Resunga Hospital of Gulmi has apparently died due to the negligence of doctors.
Shiva Lal Aryal, 53, a local of Malika Rural Municipality-6, Arje had gone to the hospital complaining of dental problem. As informed by the family members, Aryal who was taken to the hospital for normal toothache was insisted to conduct a surgery by the doctors.
Carelessness of the doctors ultimately led to his death, according to the family sources.
“Doctors had told us that a surgery needs to be conducted to take out the pus in his gums but unfortunately he didn’t wake up after the surgery,” said Hari KC, a relative of the deceased.
According to family members, the doctors were supposed to give antibiotics 24 hours before the surgery. However, they didn’t. Twenty-one-year-old son of Aryal is lying unconscious in hospital after the death of his father. Family members and relatives are refusing to claim the body accusing the doctors of the death. “We will claim the dead body only if the hospital administration along with the doctors holds a meeting with us,” said Shovakhar Giri, chairperson of Malika-6.
Tensions ran high in the hospital on Wednesday after Aryal’s death. Security personnel has been deployed at the hospital to avoid any kind of untoward incident. http://www.myrepublica.com/news/32917/
Rasunga Hospital is located in Gulmi, Palpa District.
मुख्य समाचार प्रहरीद्वारा डाक्टरमाथि हातपात, इनरुवा अस्पतालमा तनाव
Police arrest a doctor on the doctor, stress in Anirawa Hospital
मदिरामा मातिएर बुट प्रहार गरे : डाक्टर झा
Beaten the watts on the wines: Doctor Jha
काठमाडौं- दुर्घटनामा घाइते भएका आफन्तको मृत्यु भएको विषयलाई लिएर प्रहरीले डाक्टरमाथि हातपात गरेका छन् ।
KATHMANDU – Police have arrested the doctor on the subject of the death of the injured in the accident.
जिल्ला प्रशासन कार्यालय सुनसरीमा कार्यरत नायब सुब्बा रामचन्द्र भट्टरार्इ सवारी दुर्घटनामा परेका थिए । दुर्घटना लगत्तै उपचारका लािग इनरुवा अस्पताल ल्याएको थियो । अस्पतालमा कार्यरत डाक्टरले भट्टराईको अस्पताल ल्याउनुअघि नै मृत्यु भैसकेको जानकारी दिएपछि प्रहरीले डाक्टरमाथि आक्रमण गरेको बताइएको छ ।
Nab Subba Ramchandra Bhattarai, who was working in the District Administration Office, Sunsari, had been on a road accident. After the accident, brought to the hospital for treatment. According to the police, the doctor working on the hospital has died before the doctor had already died before taking Bhattarai hospital.
मृतक भट्टराईका आफन्तपर्ने जिल्ला प्रहरी कार्यालय सुनसरीमा कार्यरत प्रहरी निरीक्षक सन्तोष पोखरेलले डा तुसार झा, स्वास्थ्यकर्मी ओम गोहीबार यादवलगायत सात जना स्वास्थ्यकर्मी माथि गुण्डा सैलीमा आक्रमण गरेको प्रत्यक्षदर्शीले बताएका छन् ।
Police Inspector Satosh Pokharel, who was working at the District Police Office, Sunsari, of Bhattarai, said that the deceased was attacked by gangster Sally on the other hand, including Dr. Tusar Jha, Health Worker Om Goharbar Yadav and seven health workers.
प्रहरी निरीक्षक पोखरेलले बर्दी र बन्दुकको आडमा रक्सीमा मातेर आफूहरु माथि आक्रमण गरेको पीडित तुसार झाले बताए। अस्पतालको इमर्जेन्सी कक्षमा रहेका डा झा सहितका स्वास्थ्यकर्मी र एक जना कार्यालय सहयोगी समेतलाई बुट र लठीले कुटपीट गरेको झाले बताए।
Police Inspector Pokhrel said that according to the victim, according to the victim, attacked the victim on the side of the fire and gun. Jha said that the health worker including Dha Jha in the emergency room of the hospital and a colleague who was beaten up by robbers and robbers.
विराटनगरबाट इनरुवातर्फ आउँदै गरेको को १ च ७०३३ नं को एम्बुलेन्सको ठक्करबाट जिल्ला प्रशासन कार्यालय सुनसरीमा कार्यरत नायब सुब्बा भट्टराइको मृत्यु भएको हो ।
हिजो साँझ इनरुवाबाट आफ्नो घर दुहबीतर्फ जाँदै गरेको भट्टराई सवार बा२४प ४२४४ नंको मोटरसाइकललाई एम्बुलेन्सले ठक्कर दिँदा भट्टराइको घटनास्थलमै मृत्यु भएको प्रत्यक्षदर्शीले बताएका छन्।
Neb Subba Bhattarai, who was working in Sunsari, has been killed by Ambulance of 1 f 7033 no one coming from Biratnagar to Anwar. According to the eyelasheshi, the motorbike was beaten by Bhabhari Rider B 24 Pa 4244 in Bhattarai incident on Sunday evening.
मृतक भट्टराई आफ्नो आफन्त रहेको र सिरानी नदिएको तथा उपचारसमेत नगरिदिएको आरोप लगाउँदै डाक्टर माथि आक्रमण गरेको त्यहाँस्थित एक जना कुरुवाले प्रतिक्रिया दिए।
घटनालाई लिएर जिल्ला अस्पताल पूर्णरुपमा बन्दगरी स्वास्थ्यकर्मीहरु अस्पताल अगाडि र सडकमा धर्ना दिएर प्रहरी प्रशासनविरुद्ध नाराबाजी गर्दै प्रर्दशन गरिरहेका छन्।
A corroborate responded that the deceased Bhattarai was attacked by a doctor who was not a relative of his relatives and was not given permission and was not even treated. According to the incident, the closure of the district hospital is being done by the health workers before leaving the hospital and protesting against the police administration.
चिकित्सकमाथिको आक्रमण सह्य नहुने भन्दै इनरुवा नगरपालिकाका प्रमुख राजन मेहता, अस्पताल विकास समितिका अध्यक्ष रमेश कटुवाल, नेपाली काँग्रेका सचिव केदार भण्डारी लगायतले ऐक्बद्धता जनाउँदै चिकित्सको आन्दोलनमा सहभागी भएका छन्।
Rajan Mehta, Chairman of the Hospital Development Committee, Ramesh Katuwal, Nepali Congress Secretary Kedar Bhandari, and involvement in the movement of the doctors, said that the attack should not be done.
चिकित्सकमाथिको आक्रमणको विरोधमा सुनसरीका सबै स्वास्थ्य संस्था साँझदेखि नै बन्द भएका छन् भने दोषीलाई कारबाहीको माग गर्दै इलाम, उदयपुर, धनकुटा, पोखरा, सप्तरीलगायतका क्षेत्रमा डाक्टरले सेवा अवरुद्ध गरेको स्वास्थ्यकर्मी राजीव मेहताले जानकारी दिए।
Regarding the attack on the doctor, the health workers of Sunsari, who have closed all the health institutions of Sunsari, have been stopped from evening till demanding action against the accused, said the health service blocked by the doctors in the area of Ulam, Udaipur, Dhankuta and Saptari.
जिल्लाको पाँच वटा प्राथमिक स्वास्थ्य केन्द्रमा कार्यरत चिकित्सकले घटना सुनेपछि राति ८ः३० बजे इनरुवा आइपुगेको र आन्दोलनमा सरिक भएको डा वसन्त यादवले जानकारी दिए। उता प्रहरी र प्रशासनले आफ्नो कमजोरी भएको भन्दै मिलाउने र वार्ता गर्ने तयारी गरिरहेको बुझिएको छ।
Dr. Vasant Yadav, informed that the doctor who was working in five primary health centers in the district came to the house at 8:30 am after the incident. It is understood that the police and administration are preparing to negotiate and negotiate with their weaknesses.
Okay. I asked my trusty FaceBook friends for a condensed version of the story, and the first one wrote:
its like …there was 1 death of police man occur due to embulance while returning from market by bike…..then dead body was brought to hospital…. one of the police officer was shouting and usuing slang word to every para medics and dr …medical officer and their co worker were beaten by police … that is the scene happened….death occur in road accident….but insulting to the dr …..misbeheved …. that is life of doctor
So, this one gets added to the list. Piecing it together, a policeman was killed in a road traffic accident, (by a passing ambulance?) then the police brought his body to the hospital where he was pronounced dead. The police did not want to hear that news so they thrashed the staff and arrested the doctor on duty. I am confused as to whether the doctor on duty had anything to do with the accident (he was not driving the ambulance and was not near the scene) but – voila! – he gets arrested. I re-read the translation above and it sounds like he is accused of a crime at the scene????????
??????? help!
UPDATE: somebody explained it to me – Police inspector is the culprit and the doctor is the victim. The drunk inspector thrashed the doctor, along with others because the doctor declared the inspector’s brother in law dead on arrival, who previously met with a RTA, road traffic accident.
Now the question is: how do the police get away with this? If there is supposed to be #JailWithoutBail, who lands in the jail? the police? do they arrest themselves?
Sunsari 1 house. Sunsari district hospital has been strained after the drug-based police inspector handled over the doctor. Thursday evening at 6 pm at the hospital. On the spot of Tausar Jha, the assaulted by Inspector Satosh Kumar Pokhrel, the deceased was attacked by alcohol.
Against the protest, doctors and health workers have now stopped all the services other than accidental. To discuss this issue, the district administration is preparing to register at 10 am.
Ramchandra Bhattarai, the district administration office of the road accident, was handed over to the hospital today. But when the hospital is completed, the doctors have died. He is said to be Vinju of Inspector Pokharel.
Dr. According to Jhaka, alcohol was allegedly harassed by other doctors of the Pokharel who were earlier identified. Finally, he said that he was attacked too. I’m the only doctor here. I came to know that the inspector had to bathe. Dr. Jha said, ‘I do not go after I go.’
After the attack, the hospitals of the hospitals had abused the service including casualty last night. However, Mukunda Gautam, head of District Health Sunsari, said that the emergency service was underway. He also informed that there will be registration at District Administration at 10 am in the morning to solve the problem.
SP Vidyananda Majhi team of Sunsari had taken immediate control under the instant inspection of the hospital. The SP said that after the medical examination, the fish did not consume alcohol.
With this incident, health workers are protesting against the police administration after they are in front of the hospital and by converting on the road.
Rajan Mehta, Chief of the Municipal Municipal Hospital, Hospital Ramesh Katuwal, and affiliate said that the attack should not be done
Regarding the attack on the doctor, the health workers of Sunsari, who have closed all the health institutions in the evening, demanded treatment for the perpetrator, said the health service blocked by the doctors in the area of Ulam, Udaipur, Pokhara and Saptari and health workers Rajiv Mehta.
Dr. Vasant Yadav, informed that the doctor who was working in five primary health centers in the district came to the house at 8:30 am after the incident. It is understood that the police and administration are preparing to negotiate and negotiate with their weaknesses.
The protesters have warned that closure of the market will be closed for the indefinite period, till closing the market till Friday, as well as health institutions.
What is special?
Bhattarai died due to the collapse of Ambulance by 6 o’clock in the evening near Gonda Khela, between Sunsari Inrava- 6 and 5. He died due to the collapse of Ambulance from 1 to 7033 AH, coming from the Biratnagar to Ankara.
Bhattarai Rider, 24, 4244, who was going to Dubai from his house to Dubai, told that the incident occurred when Ambulance collapsed. He was hospitalized for treatment
(from NMA FaceBook page)
“Dr, a doctor working on INSURA Hospital on December 10, The Nepal Medical Association Central Office has been keenly concerned with the incident, according to police inspector Satosh Kumar Pokharel, who was beaten up by police, Ghali Gaulaj and other hospitals including Tussar Jha. Due to the worst condemned incident from Badriwala police inspector, all the doctors have been shocked
If such activities have been repeatedly repeatedly by the method of law and legislation, doctors and health workers can provide health services. The Nepal Medical Center, the central office, urges the police inspector to take action against such a serious situation as quickly as possible. As the police in Badri, there is no legal arrangement that can not be handled illegally.”
If there is anybody who can provide me more details, please send them. I will publish them here, anonymously if necessary. send email to joeniemczura@gmail.com
Narsinga dispatching the unkillable demon, ” Hiranyakashyapu” as depicted in a stone carving at Changu Narayan Mandir. Using a median sternotomy incision, of course. What does it take to kill something that won’t die?
O my lord, O best of the givers of benediction, if you will kindly grant me the benediction I desire, please let me not meet death from any of the living entities created by you.
Grant me that I not die within any residence or outside any residence, during the daytime or at night, nor on the ground or in the sky. Grant me that my death not be brought by any being other than those created by you, nor by any weapon, nor by any human being or animal.
Grant me that I not meet death from any entity, living or nonliving. Grant me, further, that I not be killed by any demigod or demon or by any great snake from the lower planets. Since no one can kill you in the battlefield, you have no competitor. Therefore, grant me the benediction that I too may have no rival. Give me sole lordship over all the living entities and presiding deities, and give me all the glories obtained by that position. Furthermore, give me all the mystic powers attained by long austerities and the practice of yoga, for these cannot be lost at any time.[5]
It seemed like Dr. Govinda KC needed to deliver a public tongue-lashing in order to move the process or else begin his fourteenth fast-unto-death; then finally the President of Nepal certified the ordinance governing medical education, placing a moratorium on new medical colleges in Kathmandu for the next ten years.
Success!
Um, no. Not exactly. The law promulgated is an ordinance, not a law. It is subject to confirmation when the new parliament is seated after the upcoming election.
….. The ordinance is a milestone in medical education reform, said Dr Singh. “This is one of the greatest achievements for which Dr Govinda KC was fighting since 2012, staging 13 hunger strikes till now,” he added.
The ordinance has provisioned setting up at least one government-run medical college in all seven provinces of the country within five years and places a moratorium on opening new medical colleges in the Kathmandu Valley for the next ten years.
Similarly, it has provisioned a common entrance exam system nationwide for MBBS.
Likewise, specialist doctors should serve for at least two years in remote areas or three years in the accessible areas after their completion of their studies, according to the ordinance.
Also, the government-run medical colleges should allocate 75 percent of the MBBS seats for scholarships. “Another major achievement of the ordinance is that it has provisioned formation of Medical Education Commission, which will monitor all medical colleges, and define criteria and infrastructures to operate medical colleges,” said Dr Singh. “If anyone snatches away the hard-won provisions of the ordinance from people, we will again launch appropriate movement against such move,” he added.
The Underlying Principle
The underlying principle is that medical education in Nepal needs to be supervised by doctors, not politicians, in order to maintain quality and ethical standards. Over the past five years it has seemed as though somebody is building a new medical college in Kathmandu Valley (or trying to) every few months.
If there were no limits, Kathmandu would have about twenty medical colleges, more than Delhi; London; New York; or many entire African countries.
Every young man or woman in the Valley who wanted an MBBS would be able to walk to school like they were in kindergarten.
The increase in medical colleges—mostly private and urban-centric—has very little to do with the most remote and inaccessible communities. In a country where 80% of the population lives in villages,1 medical training needs to focus on the rural population. Of the 19 medical colleges in Nepal in 2012, 14 (74%) were private and eight (43%) were in Kathmandu Valley alone, serving only 1·7 million—6% of the total population.1,6 Of the 11 medical colleges outside the Valley, almost all were based in the cities, largely depriving health care from those living in rural regions of Nepal.6
Doctors Society Of Nepal
The Doctors Society of Nepal organization published this letter:
The steps now being taken are logical and sensible but would never have happened without a champion and a movement of supporters.
Back to Vishnu
Vishnu has chosen here to appear in the form of Narasimha in order to be able to kill Hiranyakashipu without violating the boon given by Brahma. Hiranyakashipu cannot be killed by human, deva or animal, but Narasimha is none of these, as he is a form of Vishnu (a deva) incarnate as part human, part animal. He comes upon Hiranyakashipu at twilight (when it is neither day nor night) on the threshold of a courtyard (neither indoors nor out), and puts the demon on his thighs (neither earth nor space). Using his nails (neither animate nor inanimate) as weapons, he disembowels and kills the demon.[12]
It seems to me as though this tale of Narsingha is a parallel to the effort it has taken to set the path of medical education in Nepal on a proper course. Judging by the steps it took to get to this point, there will be future efforts to disregard the ordinance just like there have been efforts to ignore every previous agreement.
Finally, I don’t usually comment directly on political matters nor do I interpret Hindu beliefs. My main objective for this blog has been to promote widespread adoption of advanced resuscitation principles and training. I encourage those with other viewpoints to comment.
Unless the trend of opening medical colleges in Nepal is stopped, the country risks gaining a reputation as a “diploma factory.” The MBBS degrees awarded to young students in Nepal will not be useful in getting a medical job outside Nepal.
People don’t talk about it, but the fact is, many young medical students have the dream of going to UK, India, EU or USA to work as a doctor. It’s the best way to pay off the heavy student loans of medical college in Nepal. It’s not easy, but – it’s possible, because the medical council and the medical association are working hard to maintain some semblance of quality and accreditation.
The Nepal Medical Council and Nepal Medical Association have stood firm on the issue of quality, but are continually being challenged by politicians who wish to make money from awarding licenses to operate more and more Medical Colleges, which is lucrative due to high tuition fees and limited oversight.
Case in Point
The following article appeared in Republica Nov 6th, 2017:
KATHMANDU, Nov 6: Education Ministry has directed controversial Kathmandu National Medical College to allocate the seat numbers for new admissions from current academic calendar.
Breaching its own jurisdiction, the ministry has directed the controversial medical college to allocate the number of seats.
Though the Medical Council posses the right to allocate the seat for each academic calendar, Education Minister Gopal Man Shrestha wrote a letter to the college and directed to allot the seats.
The Senate and Executive Council of Tribhuvan University granted affiliation to the college on July 27. Later on, the university withdrew its decision to grant the affiliation citing that the college does not meet the basic requirements to operate a medical college. However, the Supreme Court, last week, issued a stay order against the decision of TU to scrap the affiliation granted to KNMC. Following the order, Minister Shrestha issued directive in writing lured with financial gain.
Nepal already has more than twenty medical colleges, with seven located in the Kathmandu Valley. ( TU, KU, Kist, NMC, NMC, PAHS).
This is from an infographic published in Republica a few years back. There is an ongoing debate about the need for new medical colleges which has been propelled by Dr. Govinda KC and which affects every aspect of medical system planning in Nepal. got o #IamwithDrGKC to find many links regarding the protests and negotiations.
This seems to be the fifth or sixth time somebody with political connections has tried to open a new medical college in the Kathmandu Valley. I am losing count!
#IamwithDrGKC
Dr. Govinda KC conducted a hunger strike – his thirteenth – not too long ago to bring attention to this issue and to pressure the government to adopt measures to prevent this. The ink on the agreement is barely dry…. and now – this.
It must be noted that a team of experts led by Kedar Bhakta Mathema, former vice chancellor of Tribhuvan University, had recommended a 10-year moratorium on establishing new medical colleges in the Valley. The original HPE Bill also had a provision for that. But under pressure from some lawmakers, particularly those from the CPN-UML and the CPN (Maoist Centre) who have stakes in some medical schools, a House committee had inserted a new clause as per which the facilities that had already obtained the letters of intent and built infrastructure would get affiliation for running the MBBS course. This would have favoured facilities like Manamohan Memorial Institute of Health Sciences and B&C Hospital among others which are backed by UML and Maoist leaders.
Nepal is a low-income nation with a population of nearly 26·5 million. The doctor–patient ratio is 0·17 per 1000 population—substantially less than the WHO recommendation of 2·3 doctors per 1000 population.1 Nepal has seen a burgeoning of medical institutes in the past 10 years. However, this rapid surge in the number of medical colleges—with increases in fees and corruption involved in student admissions—has not aided undergraduate and postgraduate medical training, deteriorating the quality of medical education.2 The financial motives involved in these private medical colleges have further incurred political meddling, often resulting in disproportionate and unregulated licensing and affiliation to such colleges, which are not instructed to establish themselves in rural areas.2,3
The increase in private medical colleges in Nepal has been a great source of debate in newspapers and national media.4 The establishment of medical colleges is often highly politicised, but repeated hunger strikes by a philanthropic activist and orthopedic surgeon, Dr Govinda KC, against the unregulated and uncontrolled accreditation of private medical colleges3 have failed to consolidate agreements made in the past. KC’s eighth hunger strike—lasting 15 days—ended on July 25, 2016, with an agreement with the government to establish medical colleges in remote regions, implement the previously drafted Mathema Committee report, abolish medical fees in government medical colleges, and depoliticise academia.3,4 The agreement, however, is still doubtful, because the government has failed to implement the past seven agreements (from seven hunger strikes), which were breached owing to political tampering from private medical colleges.3,5
The National Human Rights Commission and the Nepal Medical Association—the umbrella organisation of Nepali medical doctors—showed strong solidarity, and on July 15, 2016, issued a press release showing concern over KC’s deteriorating health and urging the government to honour their past agreements with KC.4
The increase in medical colleges—mostly private and urban-centric—has very little to do with the most remote and inaccessible communities. In a country where 80% of the population lives in villages,1 medical training needs to focus on the rural population. Of the 19 medical colleges in Nepal in 2012, 14 (74%) were private and eight (43%) were in Kathmandu Valley alone, serving only 1·7 million—6% of the total population.1,6 Of the 11 medical colleges outside the Valley, almost all were based in the cities, largely depriving health care from those living in rural regions of Nepal.6
The growth of urban-centric medical institutes does not come with a golden solution that could regulate norms and policies. The first step to revert this growing trend is to immediately consolidate the Medical Act of Nepal in line with the Mathema Committee report. The second step is to entirely depoliticise medical and academic institutions, enabling them to run under the principles of pure academia and humanitarian service. The third step is to immediately monitor the Nepalese Medical Council and university boards, and bring transparency to their decisions with stringent implementation of the rule of law.
If this is allowed, there is no end to the number of “medical colleges” that can be authorized by politicians. A Nepal MBBS degree will become worthless in the international scheme of things. Nepal risks becoming known as a “diploma mill” and will be a pariah among the system of migration for doctors to other countries in addition to not meeting it’s won needs for trained doctors.
It should be noted that one privately-owned medical college, the one in Janakpur, is already for sale after years of instability.
Update: got 280 hits in the first eight hours. Please share on FaceBook. Feel free to send anonymous stories about this topic.
At the end of my last blog, I requested readers to send stories about the incidents in which they were harassed or threatened because they were a doctor. Here is one of the replies. A doctor was harassed and it led to an arrest. It is lightly edited – I separated it into paragraphs and changed some punctuation. The write gave me permission to publish it here and I told her I would remove her name and specific reference to location.
“I am working as a MO in _____ Zonal Hospital, ______ since past 4 months on the 2 year bond through DOHS. On 2074/05/06 I along with another female MO, 2 of us were on duty in the ER, at around 11 pm a male in his mid 30’s along with his mother & wife visited the ER bringing their female relative with C/O sudden chest discomfort, was a K/C/O MR referred to Kathmandu from ______ (as far as I remember) who was going to Ktm the next day. While I was attending the patient in the dressing room (because no vacant bed was available in the ER main room) another male MO who was not on duty came to visit me for some personal work & he was patiently waiting at the dressing room door.
“Ever since they came he & his mother were complaining about the sanitation of the hospital & all. He even took pictures of the hospital boasting that he was a journalist of some kind. We kept ignoring them because if we start addressing every complain we would go crazy working here. But when he kept complaining for quite a while our male MO responded politely saying that we admit our hospital is not very clean but looking at the no of patients we receive everyday its not possible to keep it all neat & tidy at that time of night. He angrily replied that its just an excuse & if we aren’t capable of doing so we should just resign & someone worthy will replace us.
“I couldn’t resist so I intervened & said if you have any complain regarding patient care I will address it immediately but about sanitation please report to the administration next morning or being a reporter address it through your channel. Instead of listening he told me to shut up & do my job & brought out his id card boasting about being a radio station manager or something. Our male MO told me I have right to refuse seeing his patient but I didn’t feel right in making the patient suffer because of a foolish visitor like him so I left the dressing room & ordered an ECG.
“He followed me to the ER & started complaining again. I told him not to disturb my other patients he arrogantly replied that the hospital is not my personal property to stop him from talking. I asked one of the HA to inform the hospital police on duty (who usually are around the ER but sometimes go on a stroll within the hospital premises).The so called journalist now told me try not to scare him with police threat & came & sat in the chair inside the ER booth. I handed over his patient to another female MO to take 2nd opinion on the ECG from our on call consultant. I went outside the ER where our male MO was & he again followed us. Our male MO told him to stop creating a scene there but instead he said he would slap him for pointing fingers at him & verbally harassed us. Even his mother & wife couldn’t stop him from blabbering.
“Quite surprisingly all along he didn’t even cared or asked us how his patient was being treated. The hospital on duty police informed the local police & they arrested him while his mother & wife were trying to make him escape. Our another female MO on duty performed the drunkenness examination found it to be negative (no breathalyzer or any blood/urine test available in the hospital). I took a picture of the guy during that time & the police took him to the custody. I was so disturbed after this incident I couldn’t attend a single patient afterwards.
“Next day early morning we were informed he was out on bail by some another journalist who came to the hospital alone as a mediator & was asking us to compromise. We narrated the whole incident to our medical superintendent & he advised us to inform NMA far-west branch. The NMA meeting ended with the conclusion that if he is ready to apologize lets not exaggerate the matter & focus on measures to be taken to prevent such future mishaps.
“Struggling without food & sleep at around 1 pm I finally came back to my relatives house few minutes away from the hospital (as I am originally from Kathmandu & I haven’t gotten a quarter in the hospital yet) I was called to the hospital again for some emergency meeting. I rushed to the administration office but I had no idea that the so called journalist was the one who called the meeting & as soon as I entered he started demanding that I take as much time as I want but I should apologize in written for putting him in custody the whole night, for taking his picture without his consent & for using the word harassment. He was repeatedly demanding to delete his photo right in front of him. I told him I am legally unaware if its wrong to take his picture I ll find out & if it is wrong I ll apologize & delete it later but for mobilizing the hospital police & saying you verbally harassed us I won’t apologize at all.
“He now started accusing me that I am taking advantage of being a female & I unnecessarily intervened while he was arguing with our male MO last night. I told him I have every right to take a stand for my fellow staff. He & his mediator furiously stormed out saying if I don’t compromise he might file a case against me in cyber crime & for defaming him. After he left we decided to have a meeting without him the next day as in 2074/05/08 to decide how to move forward with this. So in today’s meeting almost everyone supported my decision that I should give no any written or verbal apology but I should delete his picture in his presence.& if he is apologetic lets end this matter if not we ll also fight back. Till now no any other response from the another side.
“I am still persistent on the thing that I won’t apologize under any circumstances.
Should we just accept the apology if it comes from him (which I highly doubt) & let it go or take other steps?
Is taking a photo under such circumstance legally wrong?
Is there no such thing as verbal harassment?
Is he just trying to suppress me because I am not a native from here?
Is there anything I should actually apologize for?
I replied via email to say I thought she handled it correctly. She got backup, the administrators got involved early, the police were called and removed the guy.
I will refrain from further commentary because I would like to hear from readers as to their assessment of this situation. How common is it? What to do?
If you wish your reply to be anonymous, send to joeniemczura@gmail.com and I will remove name etc before posting.
Addendum: I do want to point out that in this incident, the male M.O.s seem to have supported their colleague. The incident happened months ago, but we just finished Bhai Tika. All the males in this story deserve this:
The male colleagues of this story seem to merit a special bhai tika. sometimes we take this meaning of these ceremonies for granted. Yes, women should stand on their own two feet; but aren’t we all here to help each other?
There have been highly publicized episodes of threats and attacks against doctors in Nepal. In September the Cabinet proposed a rule change to put the burden of payment to surviving family firmly on the back of whichever doctor was involved when a patient died. This led the Nepal Medical Association to protest, and hospitals in Nepal were closed for a week this past September. The cabinet decided to delay implementing any new rule, and (among other things) a committee was formed to study the issue.
the
#JailWithoutBail
One idea that zoomed to the top was “JailWithoutBail.” It’s simple. Anybody who threatens or harms a doctor is arrested and brought to jail. Evidently this was passed in Queensland Australia several years ago. There are reports that it has not really changed anything in Queensland, and we will get to those. Even if it is an ineffective idea, time has come for serious consideration. We need to do something. We need a slogan and an easily understood plan.
In a previous blog I called for starting a database, a collection of accounts of all thrashing incidents so we could study them like epidemiology. In yet a different blog I collected newspaper accounts of thrashings so they could be read all at once. It is clear that most incidents of threats or violence do not make the news and they are not reported. At one specific hospital in Terai I was told they deal with four incidents per day in which families are unhappy, and that it is “part of the culture there” for families to be demonstrative.
We would need a bigger jail. Much bigger. That specific place deals with the problem by having better security – you can’t enter the building without going through security and you need a stick-on badge ( like they do in USA).
It is sad that there would be such a level of adversarialism, but – that is subject for another day. Denial is part of the problem – I was once told by a videshi trekking guide that there was no such problem of violence in Nepal since the Nepalese are gentle Buddhists. I would ask my readers whether they agree?
Types of confrontations and grievances
When I teach in Nepal I focus on critical care skills. Ten years ago when I first started coming here it was immediately obvious that nurses and doctors did not want to get involved and did not have the right skills when they did, so my teaching was designed to eliminate the barriers to participation. I started collecting stories about angry family members, and I have a long list of incidents which is not “scientific.”
a pregnant woman is admitted to deliver a baby and dies while in the hospital.
a political figure dies at home and the body is brought to the hospital two hours later, along with 400 members of cadre.
A family member is brought to the Emergency Room, in a critically ill condition, and the family argues with the doctor when they hear that nothing can be done or that the only alternative is expensive.
a person undergoes elective surgery and there are complications leading to death.
death of a child after admission to a pediatric unit.
Different response
sometimes a family member attacks immediately. right there in the room.
sometimes the hospital limits the visitors and sometimes not; not all Emergency Rooms are not “secure” in the same way that in-patient areas would be. Many entrances to the ER and not all are guarded.
sometimes they go and get a local political figure from one of the major parties, and then that political person gathers a crowd outside the hospital, demonstrating while the leader negotiates a cash payment to the family, while threatening to unleash the mob. (This becomes a form of extortion. There is no accounting for the proportion of the settlement that is kept by the politicians. There are reports that two-thirds of the money gets kept by the party). In Terai there was a case where the administrator of a government hospital agreed to a payment, for which no funds were available. He then cut the salary of every employee. The employees went on strike for a week, and the hospital was closed. Other hospitals experienced a flood of displaced sick people who would normally use the government hospital.
I was once told about a small hospital in the western hills where an angry mob threatened the staff after a death in childbirth, and the doctors and nurses barricaded themselves inside for five days waiting for the police to come. Finally the Army arrived and dispersed the crowd after convincing them that the local court system would take care of it. This served as part of the basis for my second book, The Sacrament of the Goddess.
The Role of the Police
I am not familiar with all the ins and outs of justice in Nepal, so I will happily accept correction. But from what I have observed, the local police captain has a large input into settling cases informally. He serves as a mediator, often conducting negotiations on the spot. In many cases, the local police captain is appointed from Kathmandu, not from the area they supervise.
Many of the incidents in which an assault takes place are over before the police are called, or before they arrive. Many hospitals do employ ghar dai, or security guards, but they are gatekeepers, not armed and do not physically intervene as a rule.
In some hospitals I am told, the police were reluctant to come and get involved in such incidents. Clearly the local captains need to be alert to a set of procedures and standing practices so they know what to do when they are mobilized. Regardless of the wording of the #jailwithoutbail law when it is promulgated, the police and APF ought to be able to work out informal ways to make sure every police agency will be sensitive to the problem.
Many of these episodes occur at night when hospitals tend to left with junior doctors while the senior doctors are sleeping at home. I have been told of two incidents where the doctor was kidnapped by a mob and brought some where else. In one of the cases, the family brought the doctor to the police; in the other, the doctor was brought to a dry paddy where he was stripped naked and given a shoe necklace. Fortunately the police arrived in force to prevent him from being burned alive, which was reportedly the nexty step.
One size does not fit all
There are some questions. Is the present system of MBBS training giving the new doctors the skills they need to deal with emergencies? Do they have enough backup from senior doctors? Are they trained to identify situations that are getting out of control?
Do the hospitals have security systems in place? what are they? How often do any of these events actually happen? Should every hospital have an actual police person on duty?
If #JailWithoutBail is adopted, when are the police called? who tells them which person to arrest? who goes to jail and when? do we wait for actual violence to occur? or just the threat? Should it be every family member present who goes to jail, or just the senior male? Should we routinely prohibit local leaders of political parties from getting involved since they tend to be the ones who gather the mob? should they be allowed to get a percentage of the settlement?
Under what circumstances does a family payout get negotiated, and who decides whether the doctor is responsible or not? For example, in some of the cases of deaths during childbirth, the woman may not have done any pre-natal visits to a doctor. Whose responsibility is that? Should there be a limit on such awards? When a death involves surgery of some kind, is it the doctor’s fault or should the actions of the entire surgical team be investigated? Not all hospitals employ the same standards of care regarding sterility of equipment, training of support staff, or availability of surgeons post-operatively.
Because of the variety of situations that may arise, any #JailWithoutBail law needs to be examined within a larger set of circumstances under which it may be applied.
Tomorrow – part two! the answers!
Write to me
I am collecting stories of thrashing incidents, please feel free to send me a story if you have one. email it to joeniemczura@gmail.com
This is provided as background to the issue of thrashing. I do not pretend that it is comprehensive. I started collecting these a few years ago and realized I need to put the list all in just one place. I will add to it. These reports will inform the reader as to the nature of the problem. Thrashing is an issue throughout Nepal.
INVITATION: if you can think of a link that needs to be added, please send it to me!
June 13 2019 two-minute-eighteen-second video compilation from various CCTV cameras showing footage of scenes of assault against doctors in India: https://youtu.be/Z9AzbKpUHlg
Dec 26, 2018 protests after death of mother and child. “सुत्केरी गराउन अस्पताल पुगेकी महिलाको बच्चासहित मृत्यु भएपछि काठमाडौंको शंकरापुर अस्पतालको वातावरण तनावग्रस्त भएको छ । सामान्य अवस्थामा प्रसूतिसेवा लिन अस्पताल पुर्याइएकी बिरामीको मंगलबार अचानक मृत्यु भएपछि बिरामीका आफन्त आक्रोशित बनेका हुन् । उनीहरुले अस्पतालमा तोडफोडसमेत गरेका छन् । (” After the death of a woman who had reached the hospital to make a complaint, the atmosphere of Shankarpur Hospital in Kathmandu has been tension. The patient’s relatives have become angry after the sudden death of the patient who was brought to the hospital for delivery in the normal condition. They have also shifted to the hospital.”) https://www.healthpostnepal.com/2018/12/26/3391/?fbclid=IwAR3MlVeDrciJqDbLa3c3Gew4PvkhBRw5sI7eRufrK8E1YRYjtcrs0ZSPYEU
Sept 23, 2018 – Rajbiraj. A toddler died (possible snakebite?) and was declared dead at the first hospital the family took him to. At the Zonal Hospital the boy was dead on arrival which the family refused to accept. A mob broke into the morgue and took the body to yet a third place. He was still dead but there was a mob protesting. http://kathmandupost.ekantipur.com/news/2018-09-23/zonal-hospital-tense-after-infants-death.html
its like …there was 1 death of police man occur due to embulance while returning from market by bike…..then dead body was brought to hospital…. one of the police officer was shouting and usuing slang word to every para medics and dr …medical officer and their co worker were beaten by police … that is the scene happened….death occur in road accident….but insulting to the dr …..misbeheved …. that is life of doctor
https://youtu.be/cCX3y3RkFJU YouTube video of news report after death of pregnant woman in Om Hospital Kathmandu. Om Hospital has also seen subsequent protests.
September 2014 Teaching Hospital (TUTH Maharajganj) report of vandalism after death of patient in dialysis unit. video in Nepali https://youtu.be/PFGfn4EMOtc
There was more news over the weekend, the bad kind of news nobody wants to read.
The Nepal Medical Association published a letter to the government:
Here is the translation, roughly. My friend in Nepal used Google translate so there are some inexactitudes in the words, but you get the idea:
Press Release
The Nepal Medical Association Central Office has focused significantly on the incident that happened on October 8, 2017 at B.P. Koirala Health Sciences Institute Dharan. Despite the tremendous efforts by the doctors after informed consent during the treatment of a patient in CCU/ICU, a patient of acute MI expired and the relatives of the patients manhandled the medical team inside CCU. The Nepal Medical Association condemns the inconvenient activities, such as handling and use of abuses on the doctors and the staffs. This union asks the government to bring legal action to the people who are taking criminal mentality to get medical attention, abusive violence, and health accidents.
The recent Mahakali Zonal Hospital, V.P., due to the incident of repeatedly handling the health institution on the doctor at impulsion and excitement, can not meditate on the sensitivity of health care, can not meditate on the actual situation, impulse and excitement. Koirala has gone to the environment in health environment, including health science establishment.
Remaining the agreement between the Nepal Medical Association for the last 24 years, the Nepal Medical Association (MoU) in the presence of the Honorable Prime Minister, for the last 20 days of amendment regarding the security of the health worker and the health organization, was given by the Nepal Physician Association for the end of the hospital and according to the purpose of handling of the patients in the hospital not only for the treatment of the patient.
The alliance The task force proposed amendment is prepared in accordance with the normal passage of the corresponding legal action in the process of re-stir the Nepal Medical Association, stern action would be compelled to note also reads.
Dr. Lochan Karki
General secretary
I think we are now entering a period in which every incident of thrashing a doctor in Nepal will be publicized.
The Kathmandu Post published the following news from Kanchanpur:
Oct 9, 2017-Service except for emergency at Mahakali Zonal Hospital in Kanchanpur has been halted from Sunday morning over health worker’s protest against an attack on them.
The entrance to the ER at Mahakali Zonal Hospital. Typical hospital construction for government hospitals in Terai.
The health workers including doctors have taken to the streets to protest an attack on them by the family of a woman, who was admitted to the hospital for delivery, and gave birth to a stillborn child on Saturday night.
The family of the mother blamed doctor’s negligence for the incident. In the attack, a police personnel deployed in the hospital was injured.
The enraged family assaulted in rage Dr Satya Prakash Koirala following the incident, said the Hospital Development Committee Chairman Ashok Pandey.
Meanwhile, the police arrested five protestors in connection with the incident. Investigations were on, said Deputy Superintendent of Police Gyan Bahadur Setti. RSS
This comes at a time when some doctors are still protesting the recent deal between NMA and the government. They do not feel adequately protected, and as a protest decided to wear motorcycle helmets during daily rounds: http://www.swasthyakhabar.com/news-details/6627/2017-10-02
Systematic data collection is needed
It is clear that a systematic registry is needed at this point. There need to be decisions made, based on the facts not sensationalized details poorly reported by the news media. The policymakers need to get more data than just what is being published. #Jailwithoutbail is a start and needs to be implemented immediately – the police role in preventing these incidents needs to be clearly spelled out. There are too many factors at play to make a clear one-size-fits-all policy.
Identify tools you might use to secure your workplace. Include physical barriers such as fences and gates, access control systems, door locks, security guards, and video surveillance.
Create a facility map that marks all doors, security cameras and stairwells. This will help law enforcement in the event of an emergency. It will also help you determine the best place to deploy security assets, such as cameras.
Devise a plan for access control. Consider using keys that cannot be replicated or cipher locks that require a code. Electronic access cards are another good option. They allow you to disable a terminated employee’s card without having to issue new codes to everyone. This system also enables management to limit access to certain areas. However, they are expensive and can be stolen. A more expensive option is a biometric system, which uses physical characteristics, like fingerprints, palm prints and iris patterns. This system is ideal for a high-security facility.
Ensure security cameras are positioned where you need them. A surveillance system can both deter criminal activity and provide valuable information about who enters and exits your facility.
Consider hiring security guards. Many facilities contract with security companies to provide guards. These guards tend to focus on screening and assisting building visitors.
Address how to secure particularly vulnerable areas. These include locations where visitors can enter freely or with little scrutiny. This might be the waiting area in a doctor’s office, the lobby of a law firm or the loading dock of a trucking company.
Conduct a periodic review of security measures. The review should ensure that doors are closed or locked as needed, that locks are functional, and that guards are properly screening visitors. For example, sometimes doors designed to keep intruders out don’t close completely, rendering their locks useless. Employees may not report this because they appreciate the convenience of not having to use their keycards. A periodic review can identify these issues and determine how your security plan should be modified to address them.
Devise a plan for communicating with employees in the event of a security emergency. If a visitor turns violent, or a fired employee returns to retaliate, what doors will you lock? How will you warn employees to seek cover? Where can they go to not only avoid harm but to escape?
Create a system for tracking security issues. If an employee reports that her ex-husband is stalking her in or around the facility, do you have a process for communicating that information to your front desk so they can watch for him? If an employee finds a door open when it shouldn’t be, does she just close it? Or does she report it so that you can investigate whether this happens a lot and adjust your security measures? The system for recording security issues doesn’t have to be complex. Purchase a simple logbook from an office supply store or record your data in a spreadsheet. Your security plan should detail where this log will be kept and who will be responsible for updating and reviewing it.
Designate a spokesperson to issue communications in the event of an incident. The spokesperson should be able to speak intelligently to the media, the public and employees’ relatives. Choose a person who would be able to impart the facts about an incident and convey concern for victims and their relatives. In more complicated situations, a public relations professional can help you craft a message for the media.
Similar advice has been reprinted here in the past. time to do it while we await action by the government.
CCNEPal, the owners of this blog, has been teaching critical care skills to doctors and nurses in Nepal since 2011 and from the beginning we included practical information as to how to minimize the threat of thrashing. The book The Sacrament of the Goddess, explores the issues surrounding thrashing as well. Since 2011, progress has been made; at least now the problem is not being ignored or swept under the rug or simply blamed on the doctor.
The hospital protest is over, and the question is whether it made any difference.
Here is the press release in Nepali from Nepal Medical Association.
I sent out a general query as to whether it was a successful protest or not. I got one particular answer I will share. It is noteworthy because the author gave a direct opinion, something very few Nepali persons will do. I have removed the name because I am not sure he wanted to become famous.
Obviously, it has been a political agenda behind the scene. Hence, it (the agreement to end protest) is not a good thing.
Demands of the majority of the doctors across the country were:
1. Jail without bail for any abuse to the health workers on duty. (Not implemented)
2. Apologize in public by the government about what they had presented at a press conference before (doctors should be liable for compensation for any death during the treatment) (Not done)
3. Determine salary of doctors scientifically (Not done) (It costs almost 5 million Nepali currency as tuition fees for Medical graduation but the current salary of a medical graduate is 30 to 35K)
4. Relaxation of retirement age of government doctor to 65 years (now it is 60 for all govt employee; some exceptions apply) and Removal of 5% health service tax was not a demand at all but NMA was focused on these two demands only. They are not going to help any doctors. This demand is focused on particular people and private hospitals
Now, what next?
Almost all the doctors who do not benefit from point 4 above are furious with NMA. some are in the opinion of establishing a parallel organization. But, one thing we doctors do not have is unity, so it will not be easy to start a fresh movement immediately.
What do i think?
Continue your days as they were before. Be careful in selecting cases. Try not to get involved in high-risk cases. I urge all the youngsters to be a member of NMA. The election will be at 3 years from now. Select a team of youngsters. Then plan ahead.
I’m writing this from USA, not Nepal, and my reading ability in Nepali is poor. But I have followed the main issue, violence against health care workers in Nepal, closely for about ten years. This has been a problem for a long time, usually swept under the rug. This past year there seem to have been more media reports of inadvertent deaths in hospitals, sensational at times. It’s an election year (there haven’t been too many elections after all) and politicians are scrambling to respond to the media reports. The media reports are generally not complete or balanced or well-researched.
Specific background to the above
If you are not familiar with the points above, let’s go point-by-point and clarify.
1. “jail without bail” is a proposal based on a law passed in 2014 in Queensland, Australia. During the Nepal protest, an internet meme made the rounds:
2. The proposal made by the cabinet which prompted the immediate protest was one in which the responsibility for patient deaths would be more clearly shifted onto the backs of the doctor(s) involved. It has yet to be put into effect, but it has not been withdrawn either. This is an ongoing issue. In my own opinion, there is need to upgrade systems of responding to emergencies, but there is also clearly a situation in which the victim or family are often portrayed as blameless in the events leading up to a death when in fact they hold some responsibility. When the political parties get involved in negotiating on the family’s behalf, it takes on the aspect of extortion.
Charikot
Here is the infamous video from the Charikot incident a year back, in which doctors were paraded in front of a crowd:
Note how young they are. And yet, they were running the place.
Another from Charikot:
This one above, gives you the idea of how volatile the protests and threats can be. A crowd has gathered and they are angry. I’m not joking when I say that this is a threat and things can get out of hand.
Another showing the crowd at Om getting whooped up, with riot police present:
What would they be doing if the police were not present? and yet, in most regions of Nepal, the police are not quick to arrive on the scene.
Here is another example of media coverage in Nepal:
The above deals with the death of a patient at Om Hospital. Let me emphasize that I personally have no any kind of inside knowledge of these specific incidents and my heart goes out the survivors. But I have in fact interviewed and worked with nurses and doctors when many other similar incidents have occurred. I firmly believe that this kind of publicity is not helping the goal to improve medical care. The doctors run away from emergencies when the family might act this way, when they ought to be running toward the emergency.
There is a definite need for more factfinding and an orderly process when an inadvertent death occurs.
3. “determine salary of medical doctors.” This needs more explanation especially for a USA audience. In Nepal they use the MBBS system. A MBBS graduate is a “doctor” after completing a Bachelor’s Degree, and they become a “Medical Officer” after completing a one-year internship. During their time as a Medical Officer there is no system to determine salary, with the result that many work three different jobs for low pay. They are continually scrounging for clinical work and under pressure to pay off medical college loans. This is one of the reasons so many wish to go to USA or UK. In addition, the young MBBS doctor often gets very little continuing education and is trapped into the role of indentured servitude, because they would need a new round of loans to enroll in the “M.D.” (i.e, master’s degree) level and finally become independent. The government sets the tuition for such graduate education but there are plenty of rumors that kickbacks are required outside the regular fee. I eould be remiss if I did not mention the work being done by Dr, Govinda KC to keep a spotlight on the need for reform of tuition at medical colleges. For that matter, there is an active effort to prevent politicians from authorizing a zillion more medical colleges in Nepal. This too, is an important quality measure.
4. retirement age of government doctors. Not an issue I personally am familiar with. Somehow this got settled when the other stated goals did not resolve. Exactly how many such persons did this affect? hmmm…….
My own recommendations for future activity
BLS, ACLS, PALS, etc need to be mandatory for all MBBS graduates during internship.
The CCNEPal project was started in an effort to improve the level of emergency care and critical care in Nepal. CCNEPal got involved in teaching about situational awareness because the fear of thrashing has always been part of the reason why emergency care is a problem. We need to continue to elevate the standards of training in emergency care procedures. The young MBBS doctors throughout Nepal are the frontline of emergency care and courses like ACLS, PALS, ATLS etc need to be mandatory for all MBBS graduates. Until now, these have been limited to only those doctors going for the Master’s degree.
2. These same courses need to be required for all MBBS graduates from China, India, Bangladesh etc
There is a significant number of MBBS graduates from non-Nepali programs working in rural areas where the care is needed most. They too need this skills even though they may not have done an internship in Nepal.
3. Nurses need this training, and it should be required for all nurses in emergency room or ICU.
4. better training and organization of ghar dai and police is also needed.
I could add a few more, and I invite you to browse previous blogs on this subject.
Last week the Nepali cabinet proposed that doctors in Nepal be responsible for compensating the family of any person that dies under their care. The Nepal Medical Association called for a “bandh” (work stoppage) in protest. Emergency rooms are open but other out-patient activities are curtailed. As of today, the bandh is still in effect. The cabinet will revisit their proposal when the Prime Minister returns from a diplomatic trip.
This is the latest chapter in a long-running problem also found in India, Pakistan and other Asian countries. Since 2011 I teach nurses and doctors in Nepal strategies to reduce the likelihood of getting thrashed.
You think of India as the home of Gandhi, right? Nepal is the land of Never Ending Peace And Love, isn’t it? Birthplace of Buddha?
At the heart of the issue is an ugly little aspect of South Asian culture. Here is what it is about:
If a patient dies while under a doctor’s care, the doctor is blamed. The family may assault the doctor, vandalize the hospital, and demand a large cash payment for the negligent care under threat of violence. Sometimes if the patient was associated with a political party, the local political chief will whoop up their cadre in a show of force to support the money demand. This form of mob justice happens throughout South Asia, to the point where it has it’s own euphemism “thrashing. (highlighting is mine, block quote added for emphasis).”
Thrashing
Thrashing is a form of frontier justice — if somebody commits a physical crime against you, you immediately convene your nearby friends with four-foot long sticks, and they join you in beating that person to a pulp.
Should doctors in Nepal carry handguns?
This is a big problem for doctors especially those serving in rural areas or in high risk specialties. In Nepal the doctors don’t want to assume this degree of personal risk. The problem is sufficiently widespread in South Asia that it has been reported by the India Correspondent of Lancet, the venerable medical journal from the U.K. and the India Medical Association proposed a bill in India’s parliament to allow doctors to carry handguns.
Political Feudalism
On another level, the local grandees of major political parties tend to get involved and will negotiate on behalf of the aggrieved party in exchange for a cut of the payout. There is a minimal malpractice system. The Nepal newspapers report on a what is now a well-publicized series of incidents in which this or that hospital gets vandalized or shut down by a mob on a rampage when there is no payout. In this blog I frequently record these incidents but they are too frequent for me to keep track of every one. The most recent seems to have been a protest at Om Hospital in Kathmandu, in which a woman died after surgery to repair a deviated nasal septum.
The above video is in Nepali. The protesters were presenting thoughtful views.
Here is another that’s a bit more raucous
I want to emphasize, I do not know the facts of the case. This particular event is added onto other recent events at the very same place, as reported in the media, and that magnifies this one. Any death of any person is tragic. Fortunately the protest after this one did not escalate into vandalism and violence.
Similar incidents have taken place at many locations, and Om Hospital is certainly not the only place!
Denial
There are many angles to the problem. One aspect is denial. As a tourist destination Nepal cultivates a certain image of happy hospitality and serenity, and this idea of thrashing does not reconcile with the image. So for a long time there has been a tendency to keep these episodes out of sight. Blame the doctor especially if they are young, but not change the system. Complicating this picture is that there is more than one level of medical training in the marketplace and there is in fact some degree of low quality medical care that qualifies as bonafide malpractice, just as we have in the USA. Also, there is a low level of medical literacy and many times the critically ill person arrives in the emergency room already dying because of delay in seeking treatment.
Life expectancy and maternal-child mortality
the life expectancy in Nepal is about 69.91 years. Maternal-Child Mortality in Nepal is high, about three times as high as that of USA despite a dramatic decrease.
This present crisis
The present brinkmanship was triggered by a proposal in Nepal’s Parliament to require that all doctors assume the cost associated with claims of malpractice. It was worded in such a way as to place 100% of the financial burden on frontline doctors. It does not address the problems of real or implied violence during the time when a resolution is being worked out. This policy if adopted, would negate the use of the judicial system to resolve these disputes which they are just starting to adopt. Here is the statement from the NMA from last week:
On their website, the Nepal Medical Association wrote:
“प्रेस विज्ञप्ति
नेपाल चिकित्सक संघ केन्द्रीय कार्यालयमा आज बसेको संघको बृहत बैठकमा उपस्थित हुनु भएका विभिन्न विशेषज्ञ समाजका अध्यक्ष तथा महासचिवहरु, अस्पताल र मेडिकल तथा डेण्टल कलेजका निर्देशक तथा संचालकहरु, संघका पूर्व अध्यक्ष, पूर्व महासचिव र संघका बरिष्ठ सदस्यहरुको भेलाले गरेको व्यापक छलफलको निर्णय बमोजिम मन्त्रीपरिषद्को मिति २०७४ आश्विन २ गते बसेको बैठकले चिकित्सकहरुलाई लक्षित गरी गरेको निर्ण…यको घोर भत्र्सना र निन्दा गर्दछ ।
आजको यस बैठकले निम्न लिखित मागहरुको सम्बोधन नभएमा यहि २०७४ आश्विन ६ गतेदेखि लागू हुने गरी देशभरका सम्पूर्ण अस्पताल, मेडिकल तथा डेन्टल कलेज, नर्सिङहोम, क्लिनिक लगायतका सम्पूर्ण स्वास्थ्य संस्थाहरुमा आकस्मिक बाहेकका अन्य सम्पूर्ण स्वास्थ्य सेवा पूर्णरुपमा बन्द गर्ने निर्णय गरिएको छ । यसको यथोचित कार्यान्वयनका लागि संघका सम्पूर्ण शाखा कार्यालयहरु, नेपाल भरीका सम्पूर्ण स्वास्थ्यसंस्था, चिकित्सक तथा स्वास्थ्यकर्मीहरुलाई यसै विज्ञप्ती मार्फत तयारी अवस्थामा रहन समेत सूचित गरिन्छ ।
तपसीलका मागहरु
१) २०७४ आश्विन २ गते बसेको मन्त्री परिषद्को बैठकले चिकित्सकहरुलाई मात्रै लक्षित गरी कानूनी राज्यको उपहास गर्दै गरिएको विवादास्पद निर्णयलाई अबिलम्ब सार्वजनिक रुपमा फिर्ता लिनु पर्ने ।
२) स्वास्थ्यकर्मी तथा स्वास्थ्य संस्थाको सुरक्षा सम्बन्धी ऐन २०६६ र नियमावली २०६९ लाई आवश्यक परिमार्जन गरी स्वास्थ्यकर्मी तथा स्वास्थ्य संस्थामाथी हातपात गर्ने व्यक्ति वा समूहहरुलाई “Jail without Bail (बिना धरौटी जेल चलान) को प्रावधानको उक्त ऐन तथा नियमावलीमा थप गर्नु पर्ने ।
३) नेपाल चिकित्सक संघसँग नेपाल सरकारले विगतका गरेका सम्झौताहरुको अक्षरस कार्यान्वयन हुनु पर्ने ।
विगतमा झै चिकित्सक संघले उठाउँदै आएको न्यायिक सवालमा समर्थनका लागि नर्सिङ, स्वास्थ्यकर्मी, नागरिक समाज, शान्ति र लोकतन्त्रका लागि पेशागत सञ्जाल (पापड), मानव अधिकार आयोग तथा संघ संगठनहरु, पत्रकारजगत तथा सम्पूर्ण बुद्धिजीवि एवं आम जनसमुदायमा यस संघ हार्दिक अपिल गर्दछ ।
नेपाल सरकारको यस्तो गैरजिम्मेवारपूर्ण निर्णयको विरुद्धमा संघबाट गरिने विरोधका कार्यक्रमबाट आम सर्व साधारणहरुमा पर्न जाने असुुविधाप्रति यस संघ दुख व्यक्त गर्दछ र यस्तो बाध्यात्मक परिस्थितिको जिम्मा नेपाल सरकार नै रहेको जानकारी गराइन्छ ।
डा. लोचन कार्की
महासचिव”
They are stating the call to close hospitals in protest, and the demands are:
1. To publicly revert the decision of the cabinet
2. Jail without bail
3. To carry out all the agreements made between the NMA and the government.
CCNEPal perspective
I am on the side of the NMA in this controversy. The proposed rule serves to blame the doctors for a very complicated situation, and does nothing to move malpractice disputes into a judicial arena. That does not mean that changes from the medical side are not needed. From my experience teaching more than three thousand doctors and nurses in Nepal about this very issue, going back six years, I have some specific recommendations.
1) mandatory adoption of courses in Nepal that cover the same content as Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) (or PEARS). All 4th year MBBS students need to be certified in this. Nepali doctors who receive their MBBS from abroad should be required to have these certifications before being licensed as a Medical Officer.
2) mandatory training of all interns and new MBBS doctors in situational awareness, counseling of patient party, and de-escalation techniques.
3) establishing a national registry of all incidents resulting in inadvertent death and thrashing or vandalism.
4) note that I agree with the “jail without bail” proposal.
5) requiring that all hospitals adopt building codes that support a controlled-access secure environment, and retrofit hospitals as needed.
6) Security personnel and local law enforcement agencies coordinate their activities.
7) Elimination of role of local political parties in negotiating settlements with local hospitals. Establishment of national fund for compensation.
8) strengthening hospital risk management systems to improve system response during sentinel events.
9) formation of a national study body to analyse trends in these incidents and share information.
Nepal is transitioning into more sophisticated medical services relying on hospitals, as opposed to the prior focus on primary care, and the educational system has not kept up with changing needs.
I encourage interested parties to browse my numerous past blogs and YouTube videos on this subject.
Interested in using your skills in an international setting for global health?
medical colleges in Nepal are working on “gender balance” but nursing is still female. The solidarity to be found in an all-female work group in Nepal is inspiring. There is an upside to go with the downside….
……. but don’t have any contacts or know where to start?
You are invited to contact CCNEPal and see if we are a fit for you for summer 2018.
We are looking for American RNs or MDs with acute care background who can help teach critical care skills to nurses and doctors in Nepal.
Time commitment: at least one month summer 2018.
budget: all expenses are borne by the participant. These typically include airfare $1500; fooding and lodging while in country ( $400 per month). tourist incidentals.
Locations: we expect to spend a bit of time in Kathmandu, the capital city, at the beginning and I will be happy to show you around. We spend time teaching in Kathmandu, but also in the Terai, the southern plains. This is not a picturesque experience distributing toothbrushes in some Sherpa Village in the Himalaya. If the location is not populous enough to support a medical college and teaching hospital, we don’t go there. Read past blogs to get an idea of where we go within Nepal.
That’s it. We will help arrange things, but we don’t charge a fee to cover some mysterious and unspecified administrative costs. CCNEPal is a shoestring operation, we expect each participant to provide their own health insurance and incidentals.
What we are looking for:
Nurses and doctors with a open mind, a sense of humor, and the willingness to work hard. This is not a party experience in any way, and I need to say upfront that if you need to have alcohol to get through the day, this is not for you. (um, caffeine is another matter. I know every source of “Organic Coffee” in every city I have visited). (instant coffee is an abomination).
What it is not:
It’s not for new graduates who do not have a solid core of acute care experience. The students can tell whether you know what you are talking about.
It’s not a sightseeing trip or party opportunity. You don’t have to work six days a week like I do (and like the Nepalis do) but there will be a full schedule of teaching in your topic arranged by our partners with full classrooms. In 2017 I taught 365 people in six weeks. you do the math.
It’s not a wander-in wander-out experience for international vagabonds with a nursing degree who wish to add Nepal to their bucket list of countries. You would need to submit a CV, letter of interest, and some references in addition to engaging in country-specific preparation.
In Kathmandu mid-morning chiya and biscuits are just the thing. Before the CCNEpal project is through, we will consume one million cups of chiya and two million biscuits. and I always ask the participants to toast – they toast the previous groups and the future groups. ( note: a few people got nescafe – OMG!)
It’s not a stay at a nice hotel with a pool. We might occasionally splurge but we mostly stay in the kind of lodging the Nepali people would favor, and we eat the local food. Don’t come if you don’t like rice.
Content and approach
We use specific teaching methods to offer a two- or three-day course in critical care skills loosely based on the AHA ACLS class (though it is emphatically NOT associated with AHA nor does it lead to a USA ACLS card). So, first and foremost we are looking for nurses who are willing to study our pedagogical approach to ACLS-type training, and teach the workshop. We don’t use PowerPoint, we don’t distribute mountains of handouts, and we don’t rely solely on lecture. We are highly practical and interactive.
We have had many inquiries to teach other courses. First, some kind of one-day workshop on nurse’s responsibilities for the mechanically ventilated patient; and second, a course in recognizing pediatric emergencies.
PALS? PEARS? ABLS? TNCC?
If you are certified to teach these, we would especially like to hear from you. There is tremendous need for these two specific courses. Similarly, ABLS (Advanced Burn Life Support).
American Heart Association
As stated above, what I teach is consistent with the latest standards of the American Heart Association, but for a long list of reasons, this is not the “official” course. Having said that, if you are qualified to teach the official course, I can forward your name to the one-and-only AHA International Training Center in Nepal and you can plan to teach with them.
Preparation:
Dal-bhaat deluxe. Rice with lentil soup is the mainstay of Nepali diet.
Nepal is not an easy country for your first international experience, and Kathmandu is not an easy first international city, if you have never travelled. Study and preparation is needed and it is important to begin months in advance. You will not be “parachuting in” – you would be working with local contacts in the health professions education sector with whom I have had working relationships for more than five years (in most cases).
About Language (and culture)
the main language of instruction in medicine and nursing in Nepal is English. However, there are many cultural nuances important to Nepal and it is helpful to study those. Even to know a little Nepali before you go, is a good idea.
This experience is ideal for a graduate student with the time to prepare. Browse through this site and related links, then give me a call.
the first Norvic “batch”included 47 people, more than usual. I had wonderful support from Kavitha Ma’am (the Matron) and Mrs. Mahima Khoju Kunwar, of the Quality department.
Packing up for a long flight
This is a quick summary of activities for summer 2017. The trip this year would not have been viable without the support of a GoFundMe campaign, to which thirteen people contributed. The campaign allowed me to buy the round trip ticket.
We were here for five weeks and taught 13 sessions to nurses and MBBS docs, in addition to two one-day classes focusing on BLS for BDS students. To be honest, there are many Nepali professionals qualified and capable to teach BLS and it was not an effective use of my time. I don’t plan to do BLS as a standalone, again.
We taught 77 nurses at Lumbini Medical College in Palpa.
Morning tea and biscuits is oh-so-civilized. I love the collegiality imparted by this small ritual. (At Lumbini Medical College).
fifty nurses at Chitwan Medical College, Bharatpur
thirtyeight nurses and MBBS (combined class) at Charak Memorial Hospital in Pokhara;
twentyseven MBBS (intern-level) at College of Medical Sciences, Bharatpur;
teamwork teamwork teamwork. The core of the training is smallgroup work to develop the ability to think on your feet during a crisis.
eightytwo MBBS (intern-level) at Chitwan Medical College in Bharatpur
One Hundred and six nurses at Norvic Hospital, Thapathali Kathmandu; and
twentyone Medical Officers at Norvic.
Total
The total seems to be 364 participants.
r screen that they are looking at a monitor screen hooked up to our Pinnacle tech AT-35. It is an invaluable tool. I left it with my colleagues at Norvic while I am away.
The Original plan was to stay until July 14th, but family concerns arose in USA and I needed to change departure dates.
When I return to USA I will focus on my job as a nursing faculty member, then starting in fall 2017 I will think about next steps for 2018. I wish to build on what I have done to create nationwide network of critical care educators. I think there is need for a nursing-focused course on mechanical ventilation as well as Pediatric Emergencies.
You are now reading the blog to accompany a project that trains Nepali nurses and doctors in critical care skills using a 2- or 3-day course based on the American Advanced Cardiac Life Support (ACLS) course. ( let me be clear: we are not the “official” course). My summer trip for 2017 is a bit shorter than usual, but we still managed to train about 350 nurses and doctors in 13 sessions ( actually, session #13 has not finished quite yet) and BLS to 40 dental students (I don’t usually teach BLS as a standalone course, but that is another story).
I teach a lot of basic skills used in critical care, including ecg. The emphasis is on applying, not just listening to lecture. we use Scenario-based simulation approach” – very active.
Future Plans
I plan to return to Nepal in 2018, and I’m thinking about what the goals would be. To some degree we are still educating people as to what ACLS is and why it is needed. We are making progress on that front, and in the planning for summer 2017 we received many more requests to partner with host sites than we could possibly fulfill.
Building Community
We’re still working to develop more Nepali professionals with the expertise and confidence to lead this course. To truly be an independent teacher of this material requires a lot of experience and confidence, more than you would be able to develop in just a weekend-long “train-the-trainer” course. There needs to be a support system to go along with it, something we take for granted in USA. A sense of community and shared purpose built around the idea that we can prevent excess deaths with better emergency response in this specific area. The people who need the training are the young nurses and docs at the bedside in off hours, and though the “seniors” need to understand it, we have to agree that the “seniors” are not really the ones who need it the most.
Most Americans have a vision of Nepal as a set of quaint villages. It’s true that much of the country is rural, but this project goes mainly to cities large enough to support a medical college and teaching hospitals.
Pediatrics
Nepal is a low income country and the profile of illnesses are not quite what you would see in USA. Read my first book, The Hospital at the End of the World, to learn more.
One theme to emerge this year was the specific need for a parallel course in pediatric emergencies. This was requested from a variety of contacts. In USA there are several such courses, the best known being “PALS” – Pediatric Advanced Life Support. So – why not?
I do not believe that PALS should be adopted widely in Nepal lock-stock-and-barrel any more than I believe that the USA ACLS course is appropriate for Nepal. First and foremost, the USA course requires that all sessions and discussions be conducted in English-only, a requirement that is simply ridiculous especially in rural Nepal. Also, the pedagogical framework of the South Asian educational system in which Nepali nurses and doctors are immersed is a consideration. These courses are at their best when they focus on practical hands-on psychomotor skills, and effective training needs to be designed with this in mind.
Invitation
Having said that, I am interested to find some people with USA acute care pediatric experience who are PALS-I (or PEARS-I, another similar course) who would be interested to come to Nepal in 2018 and teach it. Any takers?
Terms and conditions
the deal would be:
You would pay your own airfare.
You would need to commit to a month here. You would need to study the culture beforehand. No helicoptering in and out.
You would need to agree to use materials and methods appropriate to the audience. No PowerPoint, no long lectures. A good place to start exploring the approach would be the any of the sites that describes “Low Dose High Frequency” (LDHF) training. There are many, just Google the term.
You need to decide in fall 2017 whether you want to do this, because there is a lot to learn before you go the first time.
I should add that I have a friendly relationship with the Center for Medical Simulation here in Kathmandu. They are Nepal’s one-and-only American Heart Association Official International Training Center. If you want to start by teaching the American PALS course as is with no adaptations to Nepal, I am certain they would be thrilled to collaborate with you.
CCNEPal is a grassroots shoestring training operation, and we are looking for like-minded persons who wish to join us as we teach and train. Feel free to browse this site and the related links ( see the column at right). For more info send an email to joeniemczura@gmail.com.
I need to update my schedule. I cancelled all the previously-scheduled sessions outside Kathmandu Valley after June 23rd. I gave the talk in Kirtipur, and will deliver the sessions listed below. I need to do this because in USA, my father will be finishing his course of physical therapy treatments, and I will return there when he is discharged from the Rehabilitation hospital. My brother requested me to go there and so – I will return to USA three weeks early.
Here are the remaining sessions:
15. June 25th, 26th & 27th, 3-day course at Norvic (30+) ( added).
16. June 28th, 29th and 30th, 3-day course at Norvic (30+).
I added the final sessions at Norvic because they had a problem – the ones who took my sessions were extremely enthusiastic and created a sort of jealousy among those unable to register. ( some body does need to cover the patient-care duty, after all). And so we will train more persons. Also, Norvic has been “fun” and I loved the people I met there. It’s a fine hospital.
I also need to “take time and smell the incense….”
I fly out at 0815 July 2nd.
Attitude of Gratitude
I wish to extend my thanks for all the enthusiastic participants who recognize the usefulness of the courses I offer. I thrive on the positive energy. Together we can improve patient care during critical situations throughout Nepal. I hope to return in 2018 and collaborate with all my Nepali friends.
UTMB RESPIRATORY CARE SERVICES PROCEDURE – Minimal Occluding Volume (MOV) or Minimal Leak Technique Policy 7.3.49 Page 1 of 4 Minimal Occluding Volume (MOV) or Minimal Leak Technique Formulated: 11/92 Effective: 11/02/94 Revised: 11/03/14
Continued next page
Minimal Occluding Volume (MOV) Purpose
To standardize the method of minimal volume of air in the endotracheal/tracheal cuff that will allow optimal sealing of the airway.
Scope
All intubated patients will be assessed for proper volume/pressure in endotracheal cuffs with each ventilator assessment.
All tracheostomy patients not utilizing a foam-filled (bivona type) cuff volume/pressures will be monitored on a routine basis.
The acceptable intra-cuff pressure is less than 25 mmHg.
Audience
Respiratory Care Practitioners employed by the Respiratory Care Services Department with the understanding of age specific requirements of the patient population.
Equipment
10cc syringe
Stethoscope
Cuff pressure manometer
Three-way stop cock
OR Cufflator cuff inflation device
Manual resuscitator and mask
Procedure
Step
Action
1
Technique for MOV
Suction the patient airway and oral pharynx to prevent possible aspiration of retained secretions.
Place your stethoscope diaphragm over the laryngeal area and inflate cuff until all air leak is gone.
For Positive Pressure Ventilation, remove small increments (0.25-0.50cc) of air from the cuff until a small leak is heard at the point of peak inspiratory pressure (PIP). Check tidal volume to insure adequate ventilation and inflate cuff until all air leak is gone.
For spontaneous ventilation or CPAP, remove small increments of air (0.25-0.50cc) from cuff until a small expiratory leak is heard (usually in early or mid exhalation). Inflate until all air leakage is gone.
Here is a video showing exactly how to do it:
What if you use too much air?
Using the 10 cc is wrong because it causes “tracheal malacia” and post-extubation stridor. the trachea gets stretched at the point of balloon contact and collapses when air moves out. It can also contribute to tracheal-esophageal fistula. In other words, too much air in the cuff will harm the patient.
Why: “Thrashing” is a big problem in South Asia including Nepal.
Abstract: Violence against health care workers is a problem throughout South Asia and has reached a level where doctors in India have promoted an act of parliament to allow doctors to carry handguns to defend themselves. (not yet adopted). In Nepal, this issue gains publicity when sensational reports appear in the newspaper, often reaching the level of communal involvement, but the frequency seems to be seriously under-reported, and there is pressure by many stakeholders to minimize the severity of the issue. CCNEPal is a small group that delivers workshops on critical care skills to doctors and nurses in Nepal since 2011, and we include activities to raise situational awareness among young doctors to prevent difficulties with the patient party. This presentation will address the issue and share future directions to mitigate the problem in Nepal. It will take place at the D
from Kathmandu Post after a thrashing incident. These are not isolated and the problem exists throughout South Asia. Let’s talk about it.
epartment of Sociology and the media and general public are invited.
Update: This one got hundreds of hits, but few clicks on the video and I think I needed to be more focused. I made a separate entry to focus just on the ET tube cuff volume issue. CLICK HERE for the new one! http://wp.me/p1pDBL-1smBe sure to click on the video!
In this blog, the directions to ET Tube cuff volume amount are near the end. Keep reading!
I think I might do a series of blogs for nurses and Medical Officers in Nepal.
The Snake Man
Yes, that’s me but I don’t take myself as seriously as the title may imply. This is the tenth anniversary of the episode that happened in Tansen at Mission Hospital that gave me the nickname “The Snake Man” and pioneered the use of mechanical ventilation at that place. It was one of the epics of my entire life and the story is told in my first book.
In 2007 I did something that led to one of my nicknames – “the Snake Man” – you can read about it in my first book.
I didn’t actually know anything about snakes or snakebite, at the time. These days I teach about Cardiac resuscitation when I am here in Nepal, but I am sometimes asked if I would talk about nurses responsibility in mechanical ventilation. So recently I spent some time with some nurses. Instead of giving a formal talk I started off by asking questions and having them show me some things to make sure I knew what it was they were doing. I try not to re-teach people stuff they already know.
RT
For my readers not in Nepal, be advised there is no “Respiratory Therapy” profession in Nepal. Ventilators, and indeed critical care, are in the hands of “anesthesiologists” who after all, place ET tubes during surgery. Except of course when they don’t – in many small hospitals anesthesia is supplied by anesthesia technicians. So the doctors are the ones who do the vent settings.
A Canadian friend named Eric Cheng is involved with a small NGO named “Respiratory Care Without Borders,” giving workshops on this field. I don’t think he’s been back lately – RTWB now works in several dozen countries. I am going to browse their site to see what they recommend for books, etc.
This is another example of clinical issues where the nurse needs to be assertive. For example, in the USA if the tube is dislodged, the nurse removes it, uses a Bag-Valve-Mask, and calls the doc. Not every nurse in Nepal is confident or assertive enough to feel comfortable with this decision. Are you? Would you be?
Not every nurse or MBBSW doc knows how to use a BVM for that matter. I specifically require them to learn skills related to this. Including how to clean the darn thing. I wrote an eight-page policy and procedure on this a few years back.
The Pen Drive
In any case, I have decided to create another folder on the pen drive and load some documents and articles there. It’s been awhile since I updated the stuff I give to session participants. I will distribute it from now on. Bring a pen drive to class!
On the internet I found:
a Booklet titled “Mechanical ventilation for Dummies”:
How to assist at placing an Endotracheal tube (also known as “intubation”)
Here is another. This video goes over care of an endo-tracheal tube including oral care, documenting the proper depth, and repositioning:
Minimal Leak method
Cuffed ET tube
DO NOT PUT 10 cc air in ET Tube cuff. Choose the amount carefully. Use “minimal-leak” procedure:
People asked how much air to put into a cuff. I showed the group how to decide how much air goes into ET tube cuff, using “minimal leak” method. I think it worthwhile to highlight the need for this specific procedure:
Fifteen minute basic and excellent introductory lecture, first of a series:
Phasing in
There is a zen associated with effective assessment of ventilation. I always referred to this as “Phasing In” but it’s actually got a more technical name, “patient-ventilator dis-synchrony.” It’s when the patient fights the ventilator. A person on a ventilator is ideally mellow and happy; if they are not, you have to figure out why!
Here is an excellent video from Australia about “Patient Ventilator Dis-Synchrony” also known as “phasing in”
I will add to this over coming days, but – this is a start.
At Charak Hospital we do our small-group scenario practice on the roof, and it reminds me of the “Rooftop Concert” – last public performance of the Beatles.
June 7th update
We’re about to begin this year’s only session in Pokhara. This is my fifth trip here – I spent two weeks in 2016 and led five sessions. Charak Hospital is the venue, and the training hall is on the roof of the building, in full view o fthe Annapurna Range (on a good day).
For those of you new to this blog – welcome! This project began in 2011 with three goals:
train Nepali nurses and doctors in techniques of Advanced Cardiac Life Support based on the American Heart Association ACLS class (plz note that this is not the “official” class – in previous blog entries I describe in detail the hows, whys and wherefores). status: about 3,000 people have completed the course to date in about 97 sessions.
bring attention to the fact that there is such as thing as ACLS and that it is needed. Seems odd to say, but at the beginning there was tremendous resistance to the idea that the need existed. Status: Now there is wider acknowledgement of the utility of this training. Especially for nurses. This training has elevated the role of nursing at the bedside in Nepal.
create a movement within Nepal to “own” this training, not just at PG level, but during the crucial transition from MBBS to intern. It is the young doctors at bedside, often in the middle of the night or out in a rural area, who need the skills taught by this course. status: some medical colleges are sending 100% of their students to CCNEPal; others have unpgraded their training to teach in themselves. CCNEPal wrote a concept paper to strengthen the Nepal Health system and it’s right here on this blog.
You are invited to browse past entries (there are more than 200) to read all aspects of this project.
Here is the remaining schedule:
9. June 7th, 8th, 9th – 3-days course for nurses in Pokhara at Charak Hospital (38!)
June 10th – travel Pokhara back to Chitwan again. The bus goes through Tanahun, a beautiful section of Nepal.
10. June 11th, 12th; Batch #1 of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
11. June 13th,14th; Batch #2 of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
12. June 15th, 16th; – Batch three of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
June 17th – travel back to Kathmandu
13. June 18th, 19th 20th – 3-days course for nurses at Norvic Hospital (30)
June 21st reserved for special event in Kathmandu. At 3 PM that day I will deliver a one-hour guest lecture to the sociology department of T.U. in Kirtipur.
14. June 22nd 23rd, 2-days course for Medical Officers at Norvic (30)
June 24th – travel – back to Bharatpur of course!
15. June 25th, 26th – Batch #4 of four 2-days session for CMC interns (final) (30)
16. June 27, 28; 29th Nurses at Narayana Sandiak Hospital Bharatpur (30)
June 30th and July 1st – If I haven’t gone to Sauraha birdwatching by now I will surely do it. My older brother is an avid birdwatcher and I will look for them in his honor!
July 2017
17. July 2nd and 3rd – Batch #2 of three at CMS for MBBS (30)
18. July 4th and 5th _ Batch #3 of three at CMS for Medical Officers at SMC (“Purano”) (30)
revised total is about 450 if all goes as planned. Seven travel days.
19. July 6th, 7th and 8th – travel. Then two days in Kathmandu to take in the wonders of the city – to stop and smell the incense – and buy souvenirs for my friends and supporters.
20. July 9th, 10th, 11th, National Burn Center, Kirtipur (nurses) (30)
21. July 12th – 13th – National Burn Center, Kirtipur, 2-day for interns (30)
My goal is to teach until I get on the plane! I leave Nepal July 14th at 0815 in the morning from Kathmandu. My Nepal phone number is now working 98010 96822 plz don’t call after 9 PM
email me at joeniemczura@gmail.com
Dates are subject to change. If you are interested to host me or wish to clarify – my Nepali number is now working – 98010 96822 please do not call after 9 PM
1 & 2. May 18th, 19th – two one-day trainings at MC are now in the history books. 18 and 18.
May 20th – travel to Palpa
3. May 21,22, 23 – Batch #1 3-days course for nurses at Lumbini Medical College, Palpa (37, completed)
4. May 24,25, 26 – 3-days course for nurses at LMC batch #2 (39, completed)
May 27th – travel back to Bharatpur
5. May 28, 29 30 – 3-days course for nurses at CMC Bharatpur batch #1 (34)
June 2017
6. May 31st, June 1st, 2nd – 3-days course for nurses at CMC batch #2 (34)
June 3rd – day off. Maybe I will ride an elephant, maybe I will go to Sauraha and bird-watch with a guide. My elder brother loves birdwatching and has helped me to appreciate the sport. I like to keep my observation skills honed to a fine edge like the best kukri.
7. June 4th, 5th – Batch #1 of three. 2-day course at College of Medical Sciences (“Purano”) for MBBS (30)
8. June 6th – travel to Pokhara. via Mugling of course!
9. June 7th, 8th, 9th – 3-days course for nurses in Pokhara at Charak Hospital (30)
June 10th – travel Pokhara back to Chitwan again.
10. June 11th, 12th; Batch #1 of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
11. June 13th,14th; Batch #2 of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
12. June 15th, 16th; – Batch three of four 2-day session for MBBS interns and medical officers at CMC in Bharatpur (30)
June 17th – travel back to Kathmandu
13. June 18th, 19th 20th – 3-days course for nurses at Norvic Hospital (30)
June 21st reserved for special event in Kathmandu.
14. June 22nd 23rd, 2-days course for Medical Officers at Norvic (30)
June 24th – travel – back to Bharatpur of course!
15. June 25th, 26th – Batch #4 of four 2-days session for CMC interns (final) (30)
16. June 27, 28; 29th Nurses at Narayana Sandiak Hospital Bharatpur (30)
June 30th and July 1st – If I haven’t gone to Sauraha birdwatching by now I will surely do it. My older brother is an avid birdwatcher and I will look for them in his honor!
July 2017
17. July 2nd and 3rd – Batch #2 of three at CMS for MBBS (30)
18. July 4th and 5th _ Batch #3 of three at CMS for Medical Officers at SMC (“Purano”) (30)
revised total is about 450 if all goes as planned. Seven travel days.
19. July 6th and 7th are unbooked at present – I’ll be in Bharatpur…..why not?
July 8th – probable travel day, to Kathmandu.
20. July 9th, 10th, 11th, National Burn Center, Kirtipur (nurses) (30)
21. July 12th – 13th – National Burn Center, Kirtipur, 2-day for interns (30)
My goal is to teach until I get on the plane! I leave Nepal July 14th at 0815 in the morning from Kathmandu. My Nepal phone number is now working 98010 96822 plz don’t call after 9 PM
email me at joeniemczura@gmail.com
Dates are subject to change. If you are interested to host me or wish to clarify – my Nepali number is now working – 98010 96822 please do not call after 9 PM
The Ministry of Health and USAID have proposed a new project in Nepal which will focus on “Health Systems Strengthening” over a five year period. To inform the groups that will apply for the funds, USAID published a very interesting document called Notice of Funding Opportunity (NFO) describing the goals.
Three main Goals
Improved access to and utilization of equitable healthcare services
improved quality of healthcare services, and
Improved health system governance, including within the context of decentralization and federalism ( from page 6).
https://www.grants.gov/web/grants/view-opportunity.html?oppId=293419 At the beginning the NFO includes a summary of USAID-funded programs in Nepal. The portfolio of current USAID projects in Nepal was authoritatively summarized. If you are interested in the health status of Nepal, this is a must-read.
CCNEPal will not be applying
The USAID rules require that anybody applying for this grant show a track record of three prior grants of ten million USD or more, and also meet requirements to document where the money went and how the program was evaluated. For that reason, CCNEPal is not eligible to apply. Most Nepal-based entities are also ineligible unless they have a foreign partner.
What the 2017 NFO has minimized or omitted
First, a few facts. Twenty one of the proposed districts in the service area are in the Terai, the flat part of the country bordering India.
Suaahara is the main USAID project for nutrition and MCH n Nepal. This map does not depict the relative population density of the various districts.
Fifteen million people (half the population of Nepal) live in Terai. When USAID started work in Terai there were no medical colleges and few nursing colleges. USAID has worked there for years to develop nutrition programs and a system of Community Health Workers (CVHWs).
Why These areas?
This becomes easy to explain if you were to superimpose another map over the above:
Half the population of Nepal lives in Terai. All the medical schools in Terai are non-governmental, i.e., “private” – and I should add, in this region of Nepal there is a higher per centage of Hindi speakers.
Over the past ten years there is dramatic change. Today there are nine medical colleges in Terai alone, producing about three hundred and fifty new MBBS doctors per year just from this region. (there are thirteen other medical colleges in Kathmandu and elsewhere. Nepal produces about six hundred new doctors a year overall). The strategic assumptions of improving access to health care in rural Nepal as outlined in the NFO is written as if this system does not exist.
The current USAID projects are focused on Maternal-Child Health (MCH) and this proposed project will continue to focus on reducing MCH mortality.
Any plan to improve health systems strengthening needs to include the medical colleges and needs to include a plan for the doctors they produce, especially the newly-graduated doctors. A quick websearch turns up articles from WHO as far back as 1996 http://www.who.int/hrh/en/HRDJ_2_1_05.pdf that explore the idea of how many doctors Nepal needs. At that time, there were only two medical colleges in the entire country. The career path of new doctors in Nepal has been an ongoing discussion, since the government subsidizes medical education yet most new doctors are reluctant to practice in rural areas. CCNEPal has worked with newly-graduated MBBS doctors to provide confidence-building skills.
Spoke-and-wheel approach
In a decentralized (federalized) health system, the stated goal of Nepal’s Ministry of Health (MoH) and USAID is to support a spoke-and-wheel arrangement, where there is a referral center in each province and the smaller outposts refer patients to the larger center when warranted. This trend is already occurring. The flow along the spokes is conceptualized as one-way, with patients from the periphery flowing inward to each referral center. What is needed is to build a two-way system where medical knowledge is shared from the regional center outward. This is presently not happening enough.
What is the system to train new doctors in Nepal?
MBBS education is set up differently than medical school in USA.
MBBS is an undergraduate degree and is focused on reading and book work. All learning is in a very traditional classroom. There is new interest in “problem-based learning” but even this is still very didactic. Students do not incorporate “bedside manner” into their education.
Minimal clinical experience is given during the undergraduate study. A person graduates from medical college but has never written a doctor’s order, participated in an actual emergency, spoken with a nurse, or prescribed a medication let alone examined for side effects.
At graduation, a one-year internship is taken, during which the new doctor gets a crash course in practical aspects of being a doctor.
After internship, MBBS doctors become a “Medical Officer” for a year or two. Some continue as Medical Officers forever, as in government service ( “Lok Sewa”).
after a year or two of being a Medical Officer the MBBS doc goes for Post-Graduate (“PG”) training, the equivalent of a Master’s degree after which they become an M.D., also known as a Senior Doctor.
Right at this present time (2017) there is now pressure for more medical colleges to be designated as sites for PG training, as a natural consequence of turning the spigot a few years back to produce more MBBS graduates.
MBBS interns at CMC in Bharatpur. These young docs were willing and enthusiastic. A bright spot for Nepal’s future. In the recent exams, the aggregate scores for CMC were among the highest in the country.
The weak link in the chain is the internship year and the transition to being a Medical Officer. In USA, every incoming new intern would already have a CPR course, and Advanced Cardiac Life Support (ACLS) a Pediatric Advanced Life Support (PALS), and perhaps other short courses that share a hands-on practical approach to patient care. In Nepal, none of these are offered until PG training. Until recently, the model has been oriented to primary care and the idea has been that Nepali doctors do not need these skills. As Nepal transitions to a system of regional medical centers, the skill level of both doctors and nurses needs to rise. CCNEPal once estimated that to reach a level of training equivalent to western expectations, 30,000 doctors and nurses around Nepal need to upgrade their skill level with these trainings. This is a daunting scale of operation. Individual hospitals that offer these trainings are not equipped to expand programming to meet the need, and an organic system of train-the-trainer will take years to develop.
The main point is that systems need to be set in place for each medical college to address this weak link and train hundreds of persons each year. Each medical college needs incentives to promote “continuing education” for the doctors ( and nurses) in their region, that would not be the same as “PG education.” This is still a new concept for Nepal.
Health Professions Education and Research Center in Bharatpur.
CCNEPal is a shoestring operation that focuses on one thing: continuing clinical education for doctors and nurses in Nepal. CCNEPal focuses on this kind of training, but we are not the only ones who have recognized the need for continuing education at the level of intern. Chitwan Medical College (CMC) has already started their Health Professions Education and Research Center (HPERC) with the goal of providing the types of hands-on courses needed by MBBS interns as well as nurses. This was piloted in 2014 when CCNEPal trained CMC’s entire graduating batch of MBBS docs in BLS and ACLS. CMC required their entire group to take the BLS and ACLS training with CCNEPal (120 individual MBBS doctors and 90 nurses). Students reported increased confidence in decisionmaking and clinical judgement as well as willingness to take the lead in emergency situations. The CCNEPal course as presented also includes a segment on “situational awareness” that teaches counseling skills and emphasizes pro-active strategies to de-escalate during emotional situations.
What is ACLS? PALS? ATLS? NNR? AOLS?
These courses all use manikins and equipment to include psychomotor skills, teamwork skills, and knowledge of protocols in what we would call a nontraditional pedagogy approach, very different and new from the usual teaching methods of South Asia. The JHPIEGO website characterizes this as “LDHF training” – Low Dose, High Frequency. These courses teach resuscitation protocols but also impart “soft skills” of leadership, judgement, team work, communication under stress, and priority setting. These courses have been universally required in USA for decades but are still quite new in Nepal. In the past, these courses were reserved for the PG level but it is clear that first-year interns need this knowledge since they are on the front lines.
Other medical colleges have also worked with CCNEPal to train their graduates in this skill – Nobel (Biratnagar), Lumbini Medical College ( Palpa), Universal College of Medical Science ( Bhairawaha), College of Medical Sciences (like CMC, also in Bharatpur), and Janaki Medical College (Janakpur). Many have begun to investigate ways to incorporate this mode of training into skill development of nurses and doctors. Nepali MBBS graduates who trained in China also need this skill set when they return as Medical Officers in Nepal.
CCNEPal’s concept
The proposed concept is to build on the HPERC idea from CMC and expand it throughout Terai. Part of the Health Systems Strengthening grant would be used to support a system of continuing education specifically targeted at interns and medical officers who will be in the rural areas, by setting up a HPERC at four or five selected sites in Terai or rural areas associated with Medical Colleges. Each would be equipped with manikins and simulation capacity for scenario-based learning. Most of the host sites in Terai are private colleges and would need to contract with the government to train personnel from the health posts.
The Medical City of Terai
It should be noted that Bharatpur is already known as The Medical City of Terai due to the cluster of hospitals and medical colleges along with government facilities. http://wp.me/p1pDBL-1ef
What would they teach?
Each HPERC would provide training in BLS, ACLS, neonatal resuscitation, Obstetric Emergencies, ATLS, mass casualty triage, and other courses based on certifications from existing western models, including Helping Mothers Survive from JHPIEGO. https://youtu.be/Hu8Na5gqnog Each would rely on simulation equipment and scenario-based training for these short courses. Each HPERC would develop their own faculty to teach these. Each would become the hub for all nursing schools to send their students without duplicating effort ( for example, there are fourteen schools of nursing in Bharatpur alone, only two presently enroll their nursing students in ACLS).
It should be noted that in the standard B Sc nursing curriculum in Nepal, 16 hours has been allocated for ACLS training since 2008, but this is widely ignored since most nursing faculty do not know what it is or what the teaching methods entail. Nursing schools in Nepal do not have up-to-date skills labs or the system of knowledge needed to organize a skills lab. If you go to my YouTube Channel, you can view videos of nursing skills lab from around the country of Nepal. https://www.youtube.com/playlist?list=PL05C15E3E2862A608
Future course content could be developed ( for example, Nepal should consider widespread adoption of NAPPI http://nappi-training.com/ ) but the point is to develop the infrastructure for training. This cuts across all discplines. MCH personnel and critical personnel may have different clinical focus, but the training system needs to not be duplicative.
Supporting rural placement for doctors and the issue of “thrashing”
There are many issues why young doctors are reluctant to enlist in service in rural areas, and among them is the risk of harm from family members of patients who die. This is a bonafide concern, and this blog has published many entries to raise awareness of the issue. Lancet, the UK medical journal, has published a series of articles exploring the way doctors in India are coping with this as well. All new MBBS doctors in Nepal need to have training in de-escalation of anger during patient party counseling. The standard courses taught by CCNEPal since 2011 have always addressed this issue through role play and discussion.
Browsing this blog
This blog has more than two hundred entries on topics of critical care education in Nepal and the reader is invited to look at all of them.
All the props, packed up and ready to travel. CCNEPal 2016 was essentially one loooong road trip. What will we do in 2017?
Summary
CCNEPal has trained 2,885 Nepali nurses and doctors in critical care skills since 2011 with especial attention to the Terai region. We have expertise in cultural aspects of Nepal health care and health professions pedagogy that few other outside contractors can match. We offer our expertise to those leading the process of designing Health Systems Strengthening activities. We would be honored to work alongside the successful Lead Agency for this USAID project, whoever that may be.
I teach a lot of basic skills used in critical care, including ecg. The emphasis is on applying, not just listening to lecture. we use Scenario-based simulation approach” – very active.
It starts May 12th and ends July 14th
May 16th update: I leave for Terai in the morning.
My Nepal phone chip has been activated. The number is 98010 96822
To call me from USA: 011 977 98010 96822
I prefer SMS text. Do not phone or text me after 9 PM
I arrive in Kathmandu on May 12th and I’ll be in Nepal for eight weeks this time. It’s a bit shorter than last summer. The plan is to teach in Terai and western Nepal as much as I can. As before, any medical center or school interested in hosting me is invited to contact me:
joeniemczura@gmail.com
How to host
I will travel to locations outside Kathmandu if the host can do the following:
provide a class space suitable for the program. This needs to be a big space. We move around a lot during this class. It needs: 1) a whiteboard (I do not use PowerPoint) 2) thirty chairs, 3) five patient beds or trolleys for the role play scenarios. 4) air con if possible. The classroom needs to be away from a patient care area. ( we make a lot of noise).
panoramic view of classroom space. I asked them to bring the beds, for the small group work. the space was ideal for our training and I recommended to them to keep the beds there. in this ic, the groups are working on scenario practice, a key component of all such courses.
provide a roster of thirty nurses and/or doctors or MBBS students for each session of two, or three days. Nurses take a 3-day sessions and MBBS take the 2-day/ Each participant must attend all sessions of the same class to get the certificate (in other words, the three day class is a three day class – not three one-day classes). arrange for morning chiya and lunch, if there is not a cafeteria.
The sessions are for PCL nurses, B SC nurses, or MBBS. I do not register ANMs in the class. It’s okay if the person is a recent graduate, but the persons need to be working in acute care or intending to work there.
while at a place outside of KTM Valley, the host provides fooding and lodging. I live simply, it can be at a guest house, no need for finest hotel in town. I eat DBT etc so I’m okay with local food. At some locations, they lodge me in a private room on cabin ward. ( they do not need to check my vital signs though!)
My preferred schedule is to teach six days per week, either two three-day sessions (for nurses) or three two-day sessions (for doctors). I travel on Saturday and repeat. In summer 2016 I stayed two weeks in Pokhara, two in Bharatpur, two in Janakpur, and three in Biratnagar before returning to Kathmandu.
I try to make a “circuit” of sessions, not go out-and-back from Kathmandu all the time. It’s more efficient.
I supply the certificates. I keep a minimum amount of photocopy but we need about six pages per person.
My Nepali is poor ( I am ashamed to admit). Strange as it may seem, that is not an insurmountable obstacle if there are some English speakers. I adapt my teaching techniques in a certain way. If a person has no English, this may not be the class for them.
Kathmandu
I’ll try to teach at least one first-come first-registered session in Kathmandu, open to nurses that are not employed by a hospital (yet) or whose hospital is not large enough to host a session on their own.
एक वर्षभन्दा बढी समयदेखि तलब नपाएको भन्दै जानकी मेडिकल कलेजअन्तर्गत सञ्चालित शिक्षण अस्पतालका कर्मचारी आन्दोलित भएका छन् । जनकपुरस्थित शिक्षण अस्पतालका चिकित्सक र कर्मचारी काम नै ठप्प पारी आन्दोलनमा उत्रेपछि अस्पतालका सम्पूर्ण सेवा बन्द भएका छन् । ०७० सालदेखिको सबै तलब भुक्तानी, समयभित्र मासिक तलब दिनुपर्ने, करार नवीकरण हुनुपर्ने, सञ्चय कोषको व्यवस्था गर्नुपर्ने र जेएमसिटिएचको ०६४/६५ को नियमावली कार्यान्वयन हुनुपर्नेलगायत माग गर्दै कर्मचारी आन्दोलित भएका हुन् ।समस्या समाधान गर्ने विषयमा पटक–पटक कलेज व्यवस्थापनसँग सहमति भए पनि समाधान नभएपछि आन्दोलित भएको अस्पतालमा कार्यरत सञ्जय चौधरीले बताए । यसबीचमा दुईपटक सञ्चालक फेरिए पनि समस्या समाधान नभएको उनले बताए । उनले भने, ‘व्यवस्थापन सहमति गर्छ, तर समस्याको समाधान हुँदैन ।’
कलेज बिक्रीको हल्लाले कर्मचारी त्रसित
कर्मचारी दुई महिनादेखि आन्दोलित भए पनि कलेज सञ्चालन खर्च र बैंकको ब्याज असुल नहुने भएपछि बिक्रीमा राखेको एक सञ्चालक सदस्यले बताए । कलेजको ऋण १ अर्ब १० करोड र कर्मचारीको तलब करिब २० करोड बाँकी रहेको ती सञ्चालकको भनाइ छ । यस्तै, विद्यार्थीको मेस तथा अन्य खर्चबापत करिब २० करोड उधारो रहेको तथा कर, बिजुली बिल गरी करिब डेढ अर्ब रुपैयाँ तिर्नुपर्ने अवस्था रहेको ती सञ्चालकले बताए ।
कलेजको समस्या निवारणका लागि नयाँ व्यवस्थापन पक्षले कलेज बिक्रीमा राखेपछि पुराना सेयरधनी त्रसित बनेका छन् । कलेजका पुराना सेयरधनीमध्येका बलराम गुप्ता, समीर ढुंगना र उनकी श्रीमतीले सेयरबापतको करिब २५ करोड नपाएको बताएका छन् । विद्यार्थीले कलेज सञ्चालकमाथि ठगी मुद्दा दर्ता गराउने तयारी गरेपछि ढुंगना र गुप्ताले उधारोमा कलेज बिक्री गरेका थिए । कलेजलाई धनुषाबाट सार्ने तयारी भइरहेको र एक भारतीय नागरिकसँग नयाँ व्यवस्थापनले कलेज बिक्रीबारे कुराकानी गरिरहेको कलेजका एक कर्मचारीले दाबी गरे । कलेज किन्न भारतको चेन्नईबाट एउटा समूह आए पनि पूर्वाधार नभएपछि बार्गेनिङ गरिरहेको उनले बताए । यहीबीचमा भारत झारखण्डका केही व्यवसायीले पनि कलेज किन्न स्थलगत निरीक्षण गरेको उनले बताए ।
विद्यार्थीको भविष्य अन्योलमा
दुई वर्षपछि विद्यार्थी भर्ना गर्न अनुमति पाएको कलेजमा यसपटक करिब ५० जना विद्यार्थी भर्ना भएका छन् । उनीहरूमध्ये अधिकांशले किस्ताबन्दीमा शुल्क बुझाउने सहमति गरेका छन् । बुझाइएको शुल्क सञ्चालकले भागबन्डा गरिसकेका छन् । कलेज र अस्पताल सञ्चालनका लागि दैनिक खर्चसमेतको अभाव रहेको अस्पतालले जनाएको छ । तेस्रो र चौथो वर्षका विद्यार्थीले प्राक्टिकल गर्न पाइरहेका छैनन् । सिटी अस्पताल बन्द भएपछि उनीहरू बिचल्लीमा परेका छन् । कलेजका एकजना सञ्चालकका अनुसार कलेजको आम्दानीले अहिले ‘अप्रेसनल कस्ट’समेत उठ्दैन । उनले भने, ‘मासिक एक करोड ब्याज, डेढ करोड तलब, बिजुली, इन्धनलगायतका सबै खर्च धान्न महिनाको झन्डै तीन करोड चाहिन्छ ।’ अस्पताल र कलेजमा करिब पाँच सय कर्मचारी कार्यरत छन् ।
Janaki Medical College serves one of the poorest parts of Terai. There is a history of financial difficulty at JMC, and they have been on the radar of Nepal Medical Council for a number of years, charged with various action-plans to improve services.
The troubles continue. The Medical College is now for sale but nobody in the region has stepped forward with the money to invest. The asking price? 15 to 18 million USD.
I spent two weeks in Janakpur in summer 2016 to train nurses and doctors in critical care skills. If the teaching hospital is closed, that means there is only one ICU in the entire region to treat critically ill patients.
Summer 2017 CCNEPal will once again teach in Nepal.
Today we announced a new, scaled-down fundraising campaign to support CCNEPal’s summer 2017 activities. We are trying to raise $4,000 for a three-month trip to teach ACLS in Nepal, especially the areas outside the Kathmandu Valley. go to: https://www.gofundme.com/nepal-mission-for-critical-care to learn more.
This is not our first trip to the rodeo
CCNEPal has a long track record of successful training. We have taught ninety sessions of the 2-day or 3-day course in critical care skills. Since 2011 when we decided to focus only on critical care, we have given 2,885 certificates. We have trained nurses and doctors in Biratnagar, Janakpur, Chitwan, Palpa, Bhairawaha, Pokhara, Dulikhel, Manthali, and of course, in all parts of Kathmandu.
Sustainability is the goal
Our long-term commitment to Nepal has meant that we are developing a core group of people who will become teachers of this set of skills and establish a homegrown ability to pass these skills, and the attitude of critical care, to the next batch of juniors. We use a particular teaching style to empower the participants based on extensive knowledge of South Asian pedagogical style.
the group picture. the 23rd of 24 groups for summer 2016.
Shoestring budget
The funds raised by this campaign will be used efficiently. We expect to teach 24 sessions and reach about 700 nurses and doctors. That’s roughly six US Dollars per student reached. We have very little overhead. The return on investment per student is tremendous. We are not personally saving any lives – we are teaching the Nepali doctors and nurses to save the lives. We give them the tools. This is a “force multiplier” for CCNEPal’s goals.
All the props, packed up and ready to travel. CCNEPal 2016 was essentially one loooong road trip. What will we do in 2017?
This is a brief announcement.
I expect to be in Nepal once again for summer 2017. My plan is to teach more sessions of the 2-day course in Cardiac Life Support for MBBS docs and interns, as well as the 3-day course for nurses and nursing students. Please browse through back entries in this blog – there are about 240 essays on various aspects of this project. Go to the FaceBook page and browse around – you may very well know some of the 2,885 people who already took this course since 2011.
I will arrive around May 10th and return to USA around August 15th or so. The summer will mostly be a circuit trip.There are three main phases of what I expect to do:
I will land in Kathmandu Valley, run around like a crazy man gathering supplies for a couple of days, then get on a bus to Terai (or somewhere). I will settle in a location like a nomad, set up my yurt, pasture my yaks, and teach as much as I can for two weeks at a time. Similar to last year.
In the middle of the summer, one of my family members may be visiting. At that time, I will take a two-week break in Kathmandu during which I will be the guide for any and all nurses or nursing faculty who wish to learn about Nepal culture, Nepal healthcare, and Nepal nursing. During this period, I expect to focus on helping other videshis get up to speed on how they can interface with their peers, as opposed to simple sending them off to trek with toothbrushes or teach English in an orphanage. If you know of any nursing faculty for whom this might be appealing, let me know. I don’t know the dates but probably first two weeks of July (tentative).
When those persons have finished their time, I will return to Terai and resume teaching. I have this dream of visiting Beni the site of my novel; also, I wish to finally go to Jumla, the mysterious locale in western Nepal, to fulfill various solemn promises made to people long ago, some of whom are now deceased.
How to Book me?
I already got one request for me to spend two weeks in Palpa, at L.M.C. where I’ve taught before (and I also had a fine time). I do not generally construct the exact schedule of teaching too much in advance because it will inevitably change at the last minute anyway and even if it does change, I can always find people interested to work with me. (I am immensely flattered every time). So – if you are a host agency, just send me an email or a FaceBook message. I ask that the host agency pay for my lodging and fooding. I live and eat like the locals ( I admit though, Air Con is very nice when I am in Terai!)
Thousands of lives lost in the April 26th earthquake. Please pray for Nepal.
General Goal
Any Nepali nurse or doc reading this who wants to help teach and set up their own program in Nepal is strongly encouraged to contact me. This project is entering it’s sixth year, and we should be getting to the point where many people have taken the introductory course. For the skills I teach to be “sustainable” we need to think of ways to develop Nepali expertise in teaching and presentation as well as how to integrate into the ongoing curricula of nursing and medicine. If there are more requests than I can fulfill ( as has happened in previous years) I will prioritize the ones where the host can commit to finding people to adopt it in their own location with teachers that I train and then take over the content. This has happened in some places, but not others.
We have seen tremendous response to this project since it’s inception, and I hope 2017 can be just as good a collaboration as previous years.
Everything I write is based on a simple premise: If you are a medical professional from a developed country trying out #Globalhealth or #globalsurgery for the first time, you need to know as much as possible before you go. No matter how much you study, the first time is always an eye-opener. Phone me if you have questions or need advice – especially if it’s Nepal.
My belated supplement to Goats and Soda
In April 2016, Goats and Soda did a piece on a surgeon in a challenging environment.
I thought I would look through YouTube and find some other videos that put the problem in perspective. Here they are:
The Birth of the G4 Alliance
The Right to Heal
End Fistula
Aloha Medical Mission – from Hawaii – I know these guys. They are amazing. they are self-contained – bringing the whole team with them. This is one way to do it. Brad Wong, MD has also served in the capacity of being the only USA surgeon (with an all-Nepali team) on one of his trips to Nepal. I think this video below captures a lot of the team spirit:
My YouTube Channel
I take videos in Nepal when i am there, to show such things as how a nursing school learning lab is equipped. This is not the kind of thing destined to bring me viral fame but I did it for you. To see a playlist, go to https://www.youtube.com/playlist?list=PL05C15E3E2862A608
The TV show “ER”
There are many perspectives on offering your self to serve in a low-resource country. From the videos above, you get the idea of the need. There is a large gap between the medical care of USA and that of the developing world.
From the perspective of the person doing this, the person sitting down and making as rational a plan as possible before stepping out of their comfort zone, it’s an adventure regardless of which country you will go. And yes, the various possible options exist along a spectrum. The TV show “ER” did a sub-plot a few years back in which some of the surgeons-in-training went to a war zone in Africa.
As befits a dramatic series, the team is in over their heads, they are in a war zone, things go horribly wrong – actually this is the nightmare for the surgeons mother ( um, what she doesn’t know won’t hurt her. Tell her you are practicing classical piano every day like Albert Schweitzer did).
A pregnant woman died in Terai last week, and the family was overcome by grief. They showed it by angry protests. The doctor is always blamed, regardless of the facts. This is an issue that prevents young doctors from wanting to serve in rural areas. Here is more info. The news was sad for me:
Description
Alert: Chitwan/Dec 7, Birami ko mrityu pachhi aakroshit aafanta haru dwara Budhabar Chitwan Medical College ma todfod, 3 prahari sahit 4 ghaite.
The kin of a pregnant woman who died at Chitwan Medical College vandalised the hospital today.
Sunita Gurung, 25, of Bharatpur sub-metropolis was admitted to the hospital after she complained of labour pain. After Gurung died last Monday, her relatives have been staging protests saying that she died due to doctors’ negligence. The irate kin also damaged the glass of the hospital’s main door.
DSP Dipak Shrestha of District Police Office, Chitwan, said four persons, including three police personnel were injured when agitators pelted stones at the police when the latter reached the site to control the mob.
Soman Singh Gurung, family member of the deceased, said Binam Gurung was injured in the incident. Police have arrested five persons and kept them in custody for being involved in vandalism, informed DSP Shrestha.
The victim’s family, however, claimed that seven persons, including one woman were arrested. DSP Shrestha said five were held for vandalism and attack against police.
Soman Singh said Sunita was admitted in the hospital at 3:30am last Monday after she underwent labour pain.
He said Sunita died at 12 noon though the doctors had assured them that she would deliver the baby in two hours without surgery.
The deceased’s sister Gori accused that Sunita had died due to negligence on the part of doctors.
“The doctors had told us that she would deliver the baby naturally. But she lost her life due to the doctors’ negligence,” charged Gori.
The agitating kin have demanded action against guilty doctors. They submitted a memorandum to the CDO today seeking action against the guilty and compensation for the bereaved family.
Issuing a press statement today, the hospital said Sunita had died after she suddenly developed Eclampsia, a condition in which one or more seizures occur in a pregnant woman suffering from high blood pressure, and she died while being treated at the ICU.
The statement read that the deceased’s family members had signed an agreement paper on her treatment and they were informed about the complications that could develop later.
The hospital also condemned the vandalism and manhandling of doctors, nurses, and other staffers after the woman’s death.
My condolences to the victim and her family. We do not know the details of her illness, other than being “eclampsia.” The hospital is probably not allowed to release details. There is a lot we don’t know.
OBS at CMC
This is not an area I interface with as a rule. I teach people about teamwork and communication which is universal, but I do not address obstetrical emergencies per se. I don’t hang around the maternity department at any of the locations I teach.
CMC
In My opinion, CMC is among the very best hospitals in Nepal. I worked with them extensively over the past five years to address the constellation of issues related to angry patient parties who vandalize or thrash hospital staff. The reader can browse about thrity past blog entries that describe aspects of the thrashing issue. De-escalation, building design, role of security personnel, situational awareness for doctors – it’s all there.
Thrashing
This is eerily similar to the event that caused me to work on the issue of thrashing, which took place in 2009. It was very tense and became the basis of my second book, The Sacrament of the Goddess. You can buy The Sacrament of the Goddess on Amazon, here is the URL https://goo.gl/PGTW30 and there is a blog specifically devoted to the book – https://sacramentofthegoddess.wordpress.com/
Many people decide to read a book only after looking at the back cover. Here’s the one for The Sacrament of the Goddess https://goo.gl/PGTW30
As you know, I travel to Nepal to teach critical care skills to nurses and doctors. My goal is to improve the skill level and have a positive impact on health outcomes in Nepal. One of the challenges for me is that so many of the people I train take their skills to Australia or the UK or USA. I think I have trained 150 nurses now in Sydney!
The Big Question
I was very frequently asked “How can I be a nurse in USA?”
My first reaction was “Don’t. Nepal needs you, right here.”
Then after awhile, I realized I might as well put my answer in writing and refer people to this blog. It saved me time, since I no longer needed to answer the question.
“go to the blog. It’s all there.”
How to go to USA and lose your skills.
Often, the kind of person who is going to USA is a Nepali nurse who has specialized skills in Nepal and a high-status job such as in an ICU or specialty area. Now, I personally know some Nepali nurses now in USA who are, for example working in Labor and Delivery or ICU; but more often these persons accept a job in a different specialty. In USA there is a shortage of nurses who will work in Geriatrics, and many times this is where the foreign nurses work. You need to be prepared to take such a job if you can’t find the one you want.
Today’s new information to read.
I had sort of heard about the H4 visa problem, but not really paid attention until this past weekend. There was a very informative article about visa categories written by a person from India, in their blog.
Here is the problem:
If you marry a guy who is on an H1-B visa, you are given a spouse’s visa (H4) which allows you to be in USA, but specifically prevents you from working. The article described spouses from India, but it also applies to Nepali spouses.
And then there’s the huge cohort of Indian women whose careers are unravelling far away from home—in the United States of America. In the world’s biggest economy, these women are unencumbered by many of the social challenges those in India often face. Yet, their professional lives are being cut short. The culprit is a class of visa that is almost Victorian in its restrictions. (from: http://qz.com/797831/the-h4-visa-and-the-desperation-of-indian-housewives-in-america/?utm_source=KWFBUSQZ&kwp_0=273980 )
Let me be clear: this does not apply if the guy is in USA with a Green Card or if he is a citizen. I am unclear if it applies when the guy is on a J-1 visa ( i.e., a 10-year medical visa) – maybe some of the readers can help.
The entire article is well worth the read for those thinking of this route to USA.
If you go to the list of top posts from this blog (on the right of this page) you will see that the most popular ones deal with the ins and outs of leaving Nepal to work. (and of course, to see the world). You are invited to browse all of them and become an expert. If you must go abroad, you need to have your eyes open and know how to navigate.
I should add, you can address this problem by doing the extra paperwork for you own H1-B visa ahead of time, or converting over to one when you get there. But it add weeks or months to the timetable. so – be aware of it from the beginning.
Finally, if you got this far.
I have written two books, and they are both available on Amazon.
The Hospital at the End of the World https://www.amazon.com/Hospital-at-End-World/dp/1935514288 tells about my first trip to Nepal. I tried to prepare as best I could, but it was clear I didn’t really know what I was getting into. I wrote the book to inform future global nursing volunteers as to what it was like.
The second book is The Sacrament of the Goddess. https://www.amazon.com/Sacrament-Goddess-Joe-Niemczura/dp/1632100029 This one is a novel. It’s set in a hospital in Nepal during the civil war, and the people in it are forced to deal with crisis. I wanted to explore the ways that Buddhism influences choice made under stress. It’s also a honking good adventure story. Click here to browse the blog for The Sacrament of the Goddess. https://sacramentofthegoddess.wordpress.com/
You can get The Sacrament of the Goddess at Tibetan Books in Thamel.
Seems like every Nepali nurses is curious about NCLEX
A Nepali nurse-friend now in California told me she passed NCLEX, and I invited her to write a guest blog. It’s lightly edited – I broke it up into more paragraphs and added the subtitles. Look to the menu on the right and you’ll see the previous entries on this subject. Feel free to share and comment!
Hi everyone! This is Usha and guess what happened recently.. I passed the N-Clex RN. I’m so happy and I’m grateful for having studied and learning so much even though I don’t like the idea of taking test at the end. Let me introduce myself. So, I come from a beautiful city in Nepal named Pokhara and I came to United States in Aug 2014, applied for the California Board of Nursing in Jan 2015, got my ATT on Feb 2016 and here I am, finally an RN.
So now lets talk about the test. Taking the N- Clex test is stressful but you know what it’s rewarding at the end! I took off from work and joined Kaplan like 2 months before the test and started practicing questions from UWorld 3 weeks prior test. I found UWorld really helpful because it has varieties of N- Clex type questions that you can practice everyday. It also has a lot of information and diagrams inside each answers at the time of review just to make you understand in a simple way. I made notes out of it. Almost half of the questions that I had on the test were SATA, a lot of priority, one put the order, no click the spot, no drug calculation, no pictures, some meds and ECG questions. The questions are different for everyone though.
But all of these doesn’t matter. What matters is how well you can apply the things that you studied and also from your general knowledge when you answer the questions. I would also recommend nurses to know themselves first before starting to study for the test, because once you know your strengths and weaknesses, you can work accordingly and make a plan and achieve success. (Tip that worked for me during the test: Take deep breaths in between pat on your back, massage yourself on your neck, hands and legs and try to relax. Do whatever that works for you.)
Quick shut off?
It is surprising when the questions shut off at 75. You don’t know if you passed or failed. I thought I failed. But at the same time I thought if I did that bad. That evening, I applied the trick from youtube and I got a pop op saying that I’m already registered for taking the test (denotes positive result) which gave me some hope.
After 3 days I saw my name on the California board of Nursing website where it was written Usha Devkota, RN with license no. and I was shocked and had eyes full of tears. I said to myself that I did it! So yeah, life is complicated but it’s up to us to balance it out. Sometimes things can go positive and sometimes it can go wrong. But never lose hope, stay strong, believe in yourself and go on and I bet every single nurse can pass the test with handwork.
I want to thank every single person who believed in me throughout this phase. Thank you so much!
med drawer. throughout Nepal this is the standard setup. somewhere along the way everybody decided to do it this way. note that each ampule sits on cotton wadding to mitigate breakage
this is what you see when you pull out the drawer.
CMC owns more than one defibrillator, and this time aorund we used the above for training. It’s not mt favorite. The nice one ( Nihon-Kohden) was in use in their cath lab.
from the CMC website, architects drawing. Like most of the big hospitals, CMC is perpetually under construction. But they are well on their way!
Bharatpur, Nepal is located where the east-west highway intersects with the highway to Kathmandu and Pokhara. Tourists going to Chitwan National Park to see wildlife go through Bharatpur on the bus. Because of the location, Bharatpur is home to four major hospitals.
the Bharatpur District Hospitalhttp://bharatpurhospital.gov.np/, is the primary government hospital of the region and has the largest busiest maternity service in the area.
Each of these has their own sprawling complex. There are many smaller ones such as Pushpanjali Community Hospital.
There are fourteen nursing schools in greater Bharatpur.
I’m doing a series of entries on the places I teach when I am in Nepal. I’ve already described Janakpur and Biratnagar as well the National Burn Center in Kirtipur. I would be remiss if I didn’t describe the ones in this city. The challenge is, I spent a lot of time here and I know many people – it’s hard to do justice!
In general, institutions in Bharatpur do not have the kind of hosting arrangements enjoyed by some of the places in Kathmandu enjoy. They all express the interest in developing contacts. If you are from USA and you are looking for a potential partner to collaborate with, Bharatpur is a prime site for such things. Let me know.
This was new in 2016. it’s about one km from CMC.
You can get organic coffee in Bharatpur these days. When I was there in 2016, I learned that CMC is leasing space for a Lavazza coffee café just inside,off the main entrance.
site of future Lavazza coffee shop at CMC lobby floor CMC has also contracted out with a bank to put a branch on the premises, to handle all patient accounts.
the front entrance of CMC. Because CMC is at the top of the hill east of the downtown, it presents an imposing view from far away. this is close and doesn’t do it justice…
the main feature of the ground floor is an interior plaza
looking down onto the plaza from fourth floor. Judging by the uniform, these are MBBS students. It’s a grand spot for morning conference
CMC has four ICUs.
One of the ICUs at CMC. Dust is pervasive in this climate. To enter this ICU requires going through a sort of airlock that keeps the dust down
another ICU. they’ve recently reconfigured their ICUs and relocated.
surgical ICU at CMC
Nisha Bhandari is one of the senior nurses. She helped CCNEPal when we did four sessions in a row to train 120 MBBS sessions, and now she also does inservice training for other activities.
CMC’s 2016 faculty development workshop. Dr. Rano M. Piryani, is third from left in front row, he has been strong advocate for critical care skills collaboration. Mr. Siddeshwor Angadi of the nursing faculty s seated o the right end in front row, he’s my main colleague for day to day teaching.
CMC does an annual faculty development workshop for all disciplines.
Health Professional Education and Research Center.
HPERC is a new initiative of CMC. In the Nepali MBBS education system, , each batch of interns leaves for a year or two working as a Medical Officer. There is incentive for them to accept assignment in a rural or under-served area. HPERC is designed to provide Continuing Medical Education to this group, so they will more easily advance to post-graduate (PG) level and ultimately, training as a specialist with the title of “MD”
Ultimately all Medical Colleges are destined to develop a similar setup.
generally the mechanical ventilators are from European maufacturers. Like other major hospitals, CMC has four or five different models.
Nurses desk at Emergency Room
this also is well-lit and busy.
a few pictures of emergency equipment setup.
med drawer. throughout Nepal this is the standard setup. somewhere along the way everybody decided to do it this way. note that each ampule sits on cotton wadding to mitigate breakage
and another:
this is what you see when you pull out the drawer.
One of the defibrillators
CMC owns more than one defibrillator, and this time around we used the above for training. It’s not my favorite. The nice one ( Nihon-Kohden) was in use in their cath lab.
tour of fundamentals lab at CMC
tour of midwifery lab part one. Siddeshwor took me on a tour of the nursing education facilities, in a different part of town from the Teaching Hospital. I’m always interested to see what kind of learning lab they have.
tour of midwifery part two
next
On YouTube I posted a series of interviews with nursing leaders, and here is one with the Matron of CMC. In Nepali.
There are not many psyche nurses in Nepal, and Mr. Ramesh Subba is a resource.
I’ve previously described the AT-35 rhythm generator. The video below shows what it does, I took this at CMC back along. (2013)
I have more pictures of the training and the people, but I think this is enough for now. I do not conduct sessions at the District Hospital, but I have pictures of it and many of their nurses have previously taken my training when they were students at CMC or CMS.
RATNANAGAR, Oct 10: As many as 59 new cases of scrub typhus infection have been reported in Chitwan district in Asoj, pushing the number of patients in the district to 264 in the last six months.
According to the Insect Controller Inspector at the District Public Health, Chitwan, Ram Kumar KC, this bacterial disease has already claimed two lives in the district so far.
A total of eight persons have been reported dead due to the infection since its outbreak in the eastern part of the country, shared Resham Lamicchane, Public Health Officer at the Epidemiology and Disease Control Division under the Ministry of Health.
Yes. Normally I only excerpt a longer article – but that’s the whole enchilada right there.
Okay, it’s Dasain, and nobody is reading the papers and nobody is really writing any actual journalism it seems. (this blog gets noticeably fewer hits as well). Here is my problem. The article tells us there is an outbreak – that is good. But it tells nothing about what the symptoms are, how to prevent exposure, whether the treatment works, etc. They reported it, yes; but they could have also done a public service.
Fortunately we have the internet.
Here, as a public service, is some info about scrub typhus. Now, I am a person who reads about deadly infectious diseases just “for fun” and enjoyment. ( I think I need to get out more). Next, the other name for scrub typhus is – Tsutsugamushi disease. I laughed out loud, because I always loved that word. An MD friend of mine once did a locum tenans job in Brownsville Texas and told me it was endemic there – about the only place in the USA he said.
from http://emedicine.medscape.com/article/971797-overview this lesion is very closely associated with scrub typhus. When you find it, go to the hospital for antibiotics. It may be under the clothes in an uninspected area.
Preventive measures?
Preventive measures in endemic areas include the following:
Protective clothing
Insect repellents
Short-term vector reduction using environmental insecticides and vegetation control
For those who do not know the location, it is Ratnanagar – just east of Bharatpur/Narayangarh. You go through Ratnanagar to get to Chitwan National Park.
(my photo) Rush hour in Sauraha, next to Chitwan National Park. This is what the tourists see. Most cities do not actually have these.
People go through Ratnanagar but (the tourists anyway) do not stop. In Chitwan national Park one popular activity for tourists is to take a nature hike. Use insect repellant if you do.
Chloramphenicol
Interestingly, it is treatable with antibiotics. One option is Chloroamphenicol, an antibiotic no longer in use in USA. There is no vaccine.
An excellent monograph from USA’s NIH
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2829893/ this gives a technical analysis of the “laboratory bench” diagnostic tools. In the meantime, if you have a patient with febrile illness, look for the eschar; and consider the possibility of scrub typhus. In Nepal, it seems more likely in Terai, but at this time of year, people travel for Dasain, the big homecoming holiday.
something every nurse and doctor who reads this, can do.
use your smartphone to show the picture of the eschar to all your colleagues, esp if you work in a clinic or emergency room.
If your patient has recently travelled to Terai and returned to Kathmandu, be on the lookout!
the cafeteria at Norvic was restaurant quality, with a waitstaff. The canopy was covered by a blue tarp, giving it a distinctive look.
In August 2016 CCNEPal conducted a session of the three-day course at Norvic Hospital in Thapathali, a neighborhood of Kathmandu right near the river. This was not the original plan, but turned out to be fortuitous and fun.
Web page
go to http://www.norvichospital.com/ and take a look. Norvic comes with an impressive list of “firsts” – first private hospital, home of the first cardiologist in Nepal, first cath lab in Nepal, etc. The School of Nursing at Norvic has a FaceBook page https://www.facebook.com/NorvicEducations
this is not directly clinical “first” compared to angioplasty, etc. But – medical waste is a looming challenge in Nepal and Norvic seems to have designed a system for handling it. bravo!
Norvic is probably the best hospital in the country. I know I know I know, quality is elusive and arbitrary. Also I know hundreds of nurses and doctors and I should be careful not to offend anybody since there are many wonderful people who work elsewhere. Also, on each of the two occasions when I was sick or injured enough to go to the hospital, it turns out that Norvic was not where I actually went, after all. But I liked a lot of things they did, and if I were sick and had a choice, Norvic is where I would go.
In Kathmandu mid-morning chiya and biscuits are just the thing. Before the CCNEPal project is through, we will consume one million cups of chiya and two million biscuits. and I always ask the participants to toast – they toast the previous groups and the future groups. ( note: a few people got nescafe – OMG!)
I’ve not previously conducted training with them on their turf, though in the past (2013) they cycled their entire cath lab staff through my series of trainings at Lalitpur Nursing Campus. Most of the cath lab staff were new since then but several had previously taken my course.
In Norvic cath lab. lead aprons neatly stowed. ship shape!
My contact person was Mahima Khoju, RN, BSN. Mrs. Khoju got her nursing degree from the University of Texas at Arlington, back along. I think we emailed back and forth for six years before we finally met in person.
Mrs. Mahima Khoju, my contact person. If her friends from UTA could see her now…. actually, the head gear is not her usual, it’s the same puggri every body else tries on sooner or later, my favorite prop for the course.
Cath Lab at Norvic – I got the tour, but the video was cut short when the battery died.
patient care areas
one of the Medical Wards at Norvic. light and airy and dust free.
Above is the layout of the medical-surgical wards. two nurses are standing with the dressing cart. it was time for morning care, and all the drapes were pulled.
a small Newari temple in a courtyard on the premises of Norvic.
Heart Command Center
The tour focused on the ICUs in the hospital. For the Heart Command Center, one of the staff nurses gave me a specific commentary on the equipment. This is probably boring to anybody who is not an ICU nurse, but if you are? it’s dedicated to YOU!
the above gives you an idea of the equipment they have. I was interested in the external pacer box. Pacing is a thing with me. Nepal needs a more coordinated national system of how to get it for people who need it. we take it for granted in USA, but for many outlying regions if you need it you won’t get it unless you can make it to a place that has it…..
here is a poster that they still display to celebrate World Heart Day from a few years back:
sort of a re-union of heart patients.
MONA
In the ACLS protocol, “MONA” is a mnemonic device to recall certain drugs we use. I have a long-running joke about MONA, and MONA appears in my handouts. CCNEPal has trained 2,885 nurses and doctors, and only two were actually *named* Mona. So – we had a running joke for several days. Childish? mebbe. Fun? definitely!
Tokens of love
the group picture. the 23rd of 24 groups for summer 2016. probably one of the top five groups in the history of CCNEPal ( the others being MMCVTC, SHNHC, the 2011 LNC BN group, and one other whom I shall not name).
Just me and the guys
“The guys” wanted a picture. Men do not attend nursing school per se, but there is a parallel PCL course named “Health assistant” that enrolls males. I loved their attitude and sense of humor.
Haku Patasi
The final day was wrapped up with a ceremony, as always. My hosts asked me ahead of time if I had any preference for a “token of love” – and I told them. So I was delighted to be presented with two “haku patasi” and a hand-carved tea box with Ilam tea in it.
made of Nepal-grown homespun cotton, the traditional sari of Newari women. These were for my daughters. Not the usual souvenir of Nepal.
ग्रामिण क्षेत्रमा स्वास्थ्य सेवा उपलब्ध गराउँने चिकित्सकहरू को हुन् ?
नेपालमा एमबीबीएस डिग्री एउटा स्नातक तहको चारवर्षे कार्यक्रमहो जसको अन्त्यमा एक वर्षे इन्टर्नशिप गर्नुपर्ने हुन्छ।चारवर्षे यो कोर्श अत्यन्त प्राज्ञिक खालको छ र यसमा पढ्ने र परीक्षा लिने विधिमा जोड दिइएको हुन्छ। एक वर्षे इन्टर्नशिपको बेलामा मात्र युवा चिकित्सकले विरामीहरूको परिक्षण गर्ने, चिरफार गरेको हेर्ने वा त्यसमा सघाउँने अनि आदेशहरू लेख्ने गर्छन्। इन्टर्नशिप पछि ति चिकित्सकले एक मेडिकल अफिसरको रूपमा पेशा आरम्भ गर्छन् र त्यसपछि मात्र तिनिहरू स्नातकोत्तर अर्थात पोष्ट ग्र्याजुएट (पिजी) तालिम लिन जान्छन् जुन मास्टर्स डिग्री समान हो । यसले उनिहरूको नामको पछाडि एमडी उपाधि प्रदान गर्दछ। एकजना एमडीलाई वरिष्ठ चिकित्सक मानिन्छ।
‘’चरीकोट काण्ड’’
हालसालै दोलखा जिल्लाको चरीकोट स्थित अस्पतालमा भर्ना गरिएको एक बालकको मृत्यु भएको थियो। एउटा रिपोर्टले उक्त घटनालाई बिस्कुट खाँदा स्वास नली बन्द भएको भनेको थियो तर त्यसको छानविन हुँदैछ। प्रतिकृया जति यसका विवरणहरूको महत्व छैन। मृतकका परिवारले तीनसय मानिसहरूको भिड जम्मा गरे र चिकित्सकहरूलाई धम्काए। जव स्थानीय प्रशासनले भिडलाई तितरबितर पार्न सकेनन् तव उनिहरूले चिकित्सकलाई मानिसहरूको भिड अगाडि उभिएर क्षमायाचना गर्न बाध्य पारे। उक्त दृष्यको भिडियो खिचेर यु ट्युवमा प्रकाशित गरियो जुन निकै छिटो फैलियो वा भाइरल भयो जसलाई पाँच हजार भन्दाबढी मानिसहरूले हेरेका थिए।
I gave out brochures for the classes offered by my friends at the Center for Medical Simulation in Kathmandu, Nepal’s only “Official” International Training Center for ACLS with the American Heart Association
नेपालमा अल कायदा
मेडक्रोम साइटमा प्रकाशित एक समाचारमा चरीकोट भिडियोलाई अल कायदाले शरीर बन्धक बनाउँदा जस्तै तरिका उपयोग गरेको भनेर तुलना गरिएको छ। नमस्कार गरे झैँ गरेर ६ जना युवा चिकित्सकहरूलाई उभ्याइएको हेर्दा पिडा अनुभव भएको थियो। मलाई लाग्छ हरेक चिकित्सा शास्त्रको विद्यार्थीले आफूलाई अपमानित गरिएको अनुभव गरेका थिए र त्यसको मार सबैमा परेको थियो। स्वास्थ्य मन्त्रालयले उक्त घटनाको छानविन गरेर तीन दिन भित्र प्रतिवेदन दिन तीन सदस्यीय टोली पठाएको थियो।
सबैले के कुरा थाहपाउन आवश्यक छ भने यो यदाकदा मात्र हुने गरेको पृथक घटना थिएन र यसलाई त्यसरी लिइनु हुन्न। म एकजना विदेशी भएपनि म सित नेपाली नर्सिङ्को लाइसन छ र म नेपालमा हुँदा सम्वेदनशिल हेरबिचार सेवा पढाउँछु। मैले नेपालको धेरै ठाउँहरूको यात्रा गरेको छु। हजारौँ नर्स र चिकित्सकहरूले म सित कक्षा लिएका छन्। मैले नेपालमा कृतिम स्वास प्रश्वास गराउँने प्रभावकारी उपाय र अवरोधहरू माथि अध्ययन गरेको छु। यो कोर्शमा सफल परिणाम हासिल गर्नमा अवरोध गराउँने कुराहरूलाई निर्मूल पार्ने वा त्यसको सामना गर्ने तरिका सिकाउँन तयार गरिएको हो। सन् २०११ देखि नै मैले विरामीहरूका आफन्तहरूले देखाउँने गरेका आक्रामक व्यवहारलाई सम्बोधन गर्न स्वास्थ्यकर्मीहरूलाई सघाउँने तालिमलाई समावेश गरेको छु। यसमा भूमिका निर्वाह गर्ने तरिकाको उपयोग र त्यसपछि उक्त विषयमा जानकारी दिने कुरा समावेश हुनेगर्छ। म प्राय गरेर नर्स र चिकित्सकहरूसित उनिहरूले कामको सिलसिलामा यस्ता खालका भिडको प्रतिकृयाको अनुभव गरेका छन् वा छैनन् भन्नेकुरा सोध्ने गर्छु। हरेक अनुभवी चिकित्सक वा नर्सले यस्तो अनुभव गरेका हुन्छन्। त्यहाँ सयौँ कथाहरू छन् जसले तपाईँलाई स्तब्ध बनाउँन सक्छ। यो दोलखामा मात्र भएको भनेर नसोच्नुहोस – काठमाण्डुमा पनि घटनाहरू हुन्छन्। उदाहरणको लागि गत बसन्त ऋतुमा पाटन अस्पतालमा ड्युटीमा नरहेका एकजना प्रहरी अफिसरले दुईजना चिकित्सकहरूमाथि मुक्का प्रहार गरेका थिए।
चरीकोट घटना चर्चामा आएपनि त्यस्ता धेरै घटनाहरू सार्वजनिक चर्चामा आउँदैनन्। यो भिडियोका कारण सो घटनालाई वेवस्ता गर्न गाह्रो हुन्छ, र यसमा सबै चिकित्सकहरूको नाम प्रकाशमा ल्याइएको छ। यो पनि अचम्म लाग्दो कुरा छ कि स्थानीय प्रहरी यसमा असफल भएको छ। यि सबै घटनाहरू न्यायिक प्रणालीमा जानु आवश्यक हुन्छ। तपाईँले यसमा चिकित्सकहरू दोषी रहेको ठान्न पाउँनुहुन्न। उक्त अस्पतालका लागि सहयोग गर्दै आएको एउटा अन्तराष्ट्रिय एनजिओ खानेकुरा मुखमा हाल्दा स्वास प्रश्वास बन्द भएर बितेको बालकको ज्यानको लागि जिम्मेवार हुँदैन। विदेशीहरूमाथि आरोप लगाउँन सजिलो छ तर सन्चालक समितिका अधिकाँश सदस्य नेपाली नागरिक छन्।
एक निष्पक्ष छानविनले केवल दोषारोपणमा मात्र होइन त्यसभन्दा धेरै कुराको परिक्षण गर्नुपर्छ तर त्यही विन्दुमा रहेर छानविनले स्वास प्रश्वास बन्द भएको सो घटना पनि भैपरी आएको भनेर निष्कर्ष दिन सक्दैन। मेरो जानकारी अनुसार नेपालका ग्रामिण क्षेत्रमा हामीले ति युवा चिकित्सकहरूलाई पठाउँनु अघि उनिहरूलाई तयार पार्न के गर्नु पर्छ भन्नेतर्फ ध्यान दिनुपर्छ। म जहाँ जान्छु त्यहाँ म एमबीबीएसको कोर्श र इन्टर्नशिपमा पहिलो नजर लगाउँछु। मैले यो जानकारी पाएको छु कि पीजी तालिममा नजाउन्जेल नेपालमा कसैले पनि एडभान्स्ड कार्डियाक लाइफ सपोर्ट वा पिडियाट्रिक एडभान्स्ड लाइफ सपोर्टबारे अध्ययन गरेका हुँदैनन्। अधिकाँश चिकित्सा कलेज वा नर्सिङ् स्कूलमा एकमात्र सिपिआर डोल हुन्छ र नर्स तथा चिकित्सकहरूले यसको प्रयोग गरेका हुँदैनन्। उनिहरूले कृतिम स्वास प्रश्वासको लागि साइकोमोटर चलाउन दक्षता हासिल गरेको कसैले हालसम्म देखेको पनि छैन। स्षष्ट रूपमा यो खाडल वा ग्यापलाई पुर्नु आवश्यक छ। चरीकोटमा पीजी तहसम्मको योग्यता हासिल गरेका चिकित्सक थिएनन्। सबैतिर यस्तै परिस्थिति देखिन्छ। यसकारण म यो निष्कर्षमा पुगेको हुँ कि चरीकोटका चिकित्सकहरूले आफ्नो कर्तव्य निर्वाह गरेका थिए। उनिहरूले सकेसम्म राम्रोकाम गरेका थिए।
पाठ्यक्रमलाई परिमार्जन गर्नु आवश्यक छ
एमबीबीएस तालिमको चौथो बर्ष र इन्टर्नशिप वर्षलाई स्तरोन्नति गर्नु आवश्यक छ जसले गर्दा यो तालिम पुरा गर्नेहरू सबैले सफलतापूर्वक सामूहिक कृतिम स्वास प्रश्वास विधि सन्चालन गर्न सक्नेछन्। सिपिआर, एडभान्स लाइफ सपोर्ट र पेडियाट्रिक लाइफ सपोर्ट तालिम पुरा नगरून्जेल कुनैपनि चिकित्सकलाई ग्रामिण क्षेत्रमा पठाउँनु हुँदैन। नर्सहरूको हकमा पनि त्यसै गरिनुपर्छ। कुनै कुनै अस्पतालहरूमा त एकजना नर्स पनि सिपिआर दिन वा बालकको मुखमा अड्केको कुरा निकाल्न सक्षम रहेको पाइँदैन्। नर्सहरूलाई कहिल्यै तालिम दिइएको छैन। चरीकोट पनि यस्तो एउटा ठाउँ भएजस्तो लाग्छ। घटनास्थलको सबभन्दा नजिक रहने मानिसमा त्यो क्षमता हुनुपर्छ, र त्यो काम वरिष्ठ चिकित्सकहरूका लागि भनेर राख्नु हुन्न। चरीकोटमा सक्सन वा व्याग भल्भ मास्क उपलब्ध थियो वा थिएन भन्ने समेत हामीलाई थाह छैन। ति उपकरणहरू अस्पतालमा विरामी भर्ना गरिएको वार्डमा नभै आकस्मिक कक्षमा मात्र राखिनु अक्सर अनौठो कुरा होइन ।
MBBS interns at CMC in Bharatpur. These young docs were willing and enthusiastic. A bright spot for Nepal’s future. In the recent exams, the aggregate scores for CMC were among the highest in the country.
स्वास्थ्य मन्त्रालयले राष्ट्रिय स्वास्थ्य योजनामा सशोधन गर्नु आवश्यक छ मैले यो कुरा गतवर्ष प्रस्ताव गरेको थिएँ जतिबेला मैले आफ्नो कार्यक्रमलाई अगाडी बढाउँने र नर्सिङ् स्कूल र कलेजहरूलाई यो विधि अपनाउँन सघाउँने उपायहरूबारे सोचविचार गर्दै थिएँ। नेपालको राष्ट्रिय स्वास्थ्य योजनामा उल्लेखित ति दक्षताहरू समावेश नभएसम्म लगानी खोज्नका लागि कुनै पनि काम कारबाही नगरिने कुरा थाह पाउँदा म अचम्म परेको थिएँ। त्यसो होइन। थप कुरा के हो भने उक्त योजनालाई अध्यावधिक गर्न सघाउँन सक्ने अधिकाँश प्रशासकहरूलाई कृतिम स्वास प्रश्वास भनेको के हो भन्नेकुराको समेत यकिन जानकारी छैन्। न त यसलाई प्रभावकारी रूपमा सिकाउँन अबलम्बन गरिनुपर्ने विशेष सिकाई विधिबारे नै जानकारी छ। मेरो आफ्नै कोर्समा पनि नकारात्मक परिणाम आउँदा बखत हामी परिस्थितिलाई चर्कन नदिएर मत्थर पार्ने कला सिकाउँछौँ अर्थात त्यसबारे काउन्सिलिङ् गर्छौँ। चीनमा एमबीबीएस अध्ययन गरेका नेपाली विद्यार्थीले प्रयोगात्मक दक्षता हासिल गर्ने मौका अझ कम पाउँछन्। यस्ता तालिमको कमिका कारण नेपालमा तालिमप्राप्त गरेका चिकित्सकहरूका लागि भारतमा वा अन्य देशमा थप विशेषज्ञता हासिल गर्न हुने प्रतिस्पर्धामा नाम निकाल्न अझ गाह्रो हुन्छ।
यदि स्वास्थ्य मन्त्रालयले राष्ट्रिय स्वास्थ्य योजनाको लक्ष्य अध्यावधिक गरेर कृतिम स्वास प्रश्वास क्षमतामाथि ध्यान केन्द्रित गरेर चिकित्सा कलेजको पठन पाठन वा इन्टर्नशिप वर्षमा त्यसलाई समावेश गरेमा यो क्षेत्रमा विदेशी लगानी निर्देशित हुने सम्भावना रहन्छ र नेपालको लागि यस्तो लगानीको प्रतिफल लाभदायक हुनेछ। आगामी वर्षहरूमा नेपालले नयाँ चिकित्सकहरूलाई दूर दराजका ग्रामिण क्षेत्रहरूमा चिकित्सा सेवा उपलब्ध गराउँने उपाय स्वरूप ति ठाउँहरूमा पठाउँने सोच विचारलाई निरन्तरता दिनेछ। हामीले उनिहरूलाई सफल तुल्याउँने र सुरक्षित रूपमा काम गर्नसक्ने बनाउँने क्षमता भरिदिनु पर्छ। समस्या समाधानका लागि यो एकमात्र रणनीति होइन तर यो एउटा महत्वपूर्ण कदम हो।
Joe Niemczura, RN, MS अमेरिकाबाट आउँनु भएको हो र उहाँले नेपाली नर्सिङ्को लाइसन प्राप्त गरिसक्नु भएको छ। उहाँ CCNEPal मा Principal Faculty हुनुहुन्छ र उहाँले आफ्नो कोर्शको सिलसिलामा ९० वटा क्लास मार्फत २८८५ नर्स र चिकित्सकहरूलाई पढाइसक्नु भएको छ। उहाँको दोश्रो पुस्तक –The Sacrament of the Goddess एउटा उपन्यास हो। यसमा शिशु जन्माउँने क्रममा नचाहँदा नचाहँदै ज्यान गुमाएकी एकजना आमाको मृत्युको विषयलाई लिएर क्रुद्ध भिडले चिकित्सकमाथि गरेका दूर्व्यवहारको कहानी उल्लेख गरिएको छ। Niemczura ले नेपालमा स्वास्थ्य सेवा क्षेत्रमा कामगर्ने मानिसहरू विरूद्ध हुने गरेका हिँसाबारे गहन अध्ययन गरेर त्यसलाई उपन्यासमा उतार्नु भएको छ। त्यसबारे थप जानकारी Amazon वा Vajra Books ठमेलबाट पाउँन सकिन्छ। थप जानकारीको लागि उहाँको ब्लगwww.joeniemczura.wordpress.comमा हेर्नुहोस्।
The post below was written shortly after I learned of the events in Charikot. Turns out the patient was two-and-a-half years old, not a newborn. There have been other developments – all the doctors have left; the local political authorities did not seem to have taken the proper action; the video has been roundly condemned; the hospital is presently shutdown; and the family has expressed the idea that they did not want such a drastic outcome. The Ministry of Health has sent a three-person committee to Charikot.
It’s more than I can keep up with. I need to resist the urge to relay each new development breathlessly before the next step develops.
For me, the bottom line remains that the young doctors needed more preparation for their posting, then they got. For five years I have worked to promote the need to teach situational awareness. I am hoping that if there is any good to be gained from, it will be when the Ministry of Health, The Nepal Medical Association, and the medical colleges take a good look at how to introduce this into the curriculum for all MBBS doctors in Nepal.
Charikot Incident
In Charikot, Dolkaha district of Nepal, the hospital staff are under investigation due to an incident in which a newborn baby (correction: 2 1/2 year old) died after being brought to ER. It is not unusual to have a person die in an Emergency Room; in this case the family reacted by blaming the hospital staff and threatening them. This too, is not unusual. Any Nepali nurse can tell you this or that incident in which this was a problem.
In Charikot, none of the staff seem to have been hurt (we await more details) but the whole incident was traumatic. The local authorities are investigating.
I’ve been through Charikot, on a “local” bus. It was the last east-bound bus of the day. We were all headed to Manthali. http://wp.me/p1pDBL-pK The bus was overfull. Such buses always are. The bus crew did not want anybody on the roof. About a dozen guys wanted to ride the roof. There was an argument and a lot of shouting and jostling. The guys got on. Rural Nepal is not always Never Ending Peace and Love.
Back to the incident at hand
start with a recent video:
(update: evidently the acting district officer was unable to disperse a crowd of 300 people who had gathered, and ordered the doctors to do this, recording this video. This is unprecedented in Nepal). The hospital in Charikot was damaged in the second big earthquake of 2015, May 6th, when the epicenter was in Dolakha district. Since then, it has been a project of the US-based NGO, “Possible Health.”
Here is the website of Possible: http://possiblehealth.org/rebuilding-nepal/ They are doing good work in a critical sector. The NGO is “foreign” but the staff is Nepali. ( update: and most of the members of their Board are Nepali).
The link above includes a description of their work in Charikot and rebuilding health posts in that region. There is an informative Q & A.
Press Release
Since the incident, there is a press release from Possible Health:
This describes the incident. In Nepali of course! I do not presently have an exact translation.
My friends from Possible were shocked.
For me, the story is familiar. A critically ill person is brought to the ER. The family demands the staff to do something, but it is too late and the victim dies. Somehow the family demands that the staff be held responsible. Things spiral out of control.
A lot of my work in Nepal is to prepare nurses and doctors for appropriate handling of this situation, and in fact, CCNEPal has trained 2,885 nurses and doctors as to how to respond when this exact thing happens. We do this by incorporating a scenario-based approach to the principles of counseling the patient party.
Critical fact!!!!!!!
This happens all over Nepal. It is not the first time. It is more highly publicized than most of the other times.
One important thing to know is – the doctor(s) will always be blamed regardless of the facts of the case. Anger is a predominant response in acute grief in Nepal. These incidents have a history of happening throughout the country and they are depressingly familiar.
next, on this very blog are a dozen or more entries on the subject of how to
prevent thrashing and to maintain an secure environment.
MBBS students participating in a role play. Here, they are security guards bringing an unresponsive “victim” for emergent care. Other participants play the role of distraught family.
at the end of the time in Biratnagar, the farmers planted the entire paddy behind the guest house, as well as others. during this period, it’s like the hospital is an island in a large lake that’s only six inches deep. I left one day before the torrential rains began for monsoon 2016.
Thirty million people live in Nepal, and 99.999999999% of them do not live anywhere near Everest. Nepal also has a large rice-growing region, where western tourists are rarely seen. See the above photo!
Since 2011, CCNEPal works on a project to improve health care for those people.
Maybe that’s a little vague. Try this:
Imagine a hospital with no Code Blue team. Nobody knows CPR, they don’t do “Rapid Response Teams” and if a patient crashes due to a predictable complication after routine surgery, it’s a hit or miss proposition as to the outcome. That’s the situation for most hospitals in Nepal.
It’s easy to say “Oh, it can’t be helped. Nepal is a low income country after and they are used to a short life span.”
CCNEPal’s answer? Yes it can be helped! Our answer is simple: we teach critical care skills in a two- or three-day intensive course based on the ACLS course of the American Heart Association (we adapted the content to fit Nepal and it is not the “official” course). As of Dec 2018, we have taught a hundred twenty sessions, and given certificates to nearly 4,000 nurses and doctors across many regions of Nepal. We have created widespread awareness of the training and recognition of the need for this training after five years of work.
In 2019 the plan is to build on this work. I have been looking for a trendy name. So – I decided to try out The Himalayan Zap Trek 2019 was born.
What is a “Zap Trek”?
“Zap” is the sound made by a defibrillator when you shock a dying patient. (actually, “zork” is a more accurate term, but “zap” is used by doctors and nurses worldwide, so zap it will be). “Zap” is an onomatopea.
Nurses: A Force for Change: Improving Health Systems’ Resilience
above is the title of the Oct 14th and 15th 2016 meeting of Boston’s Global Health Nursing Caucus (in Boston of course!) and the event can be found at:http://seedglobalhealth.org/nursing-conference/#.V96VLIf2Zjo It’s co-sponsored with SEED Global Health.
Lightning Talks between 11 and 12:30 the 15th
They’ve made space for “lightning talks” – five to ten minute presentations modeled after the popular “Ted Talks” – a chance for the speaker to present just one idea. This is a great idea – the best meetings are ones where you can learn from the other attendees as much as from the presenters. This gives people the chance to figure out who is in the audience next to them.
these ladies are wearing “paranda” – a traditional tassel or hair extension. I got a lot of these for the C.U.G.H. meeting last spring.I have some remaining and I’ll bring them. Want one? just ask!
The Three-Legged Stool of Global Health Nursing
That’s the title of my lightning talk. I needed to focus on just one idea, and that’s what I chose. It’s the most elegant way to think of how to advance nursing in Low Income Countries. Some projects succeed, some fail. Sometimes you see things that you want to change, and which can’t be changed no matter what you try to teach or do or model or support.
The three legs compose a “Schema” of interrelated phenomena. If you try to change one, without addressing the other two, your stool will not be level, and may collapse when you try to sit on it…….
First leg is culture and the role of women.
medical colleges in Nepal are working on “gender balance” but nursing is still female. The solidarity to be found in an all-female work group in Nepal is inspiring. There is an upside to go with the downside….
Second Leg is the nursing education curriculum and system.
seen on a classroom whiteboard of a PCL nursing school in Kathmandu, Nepal. Students there are regimented; they learn to love it, and even if they don’t it molds them a certain way…..
Study the above! ( don’t confuse it with the argument about “functional vs. dysfunctional,” that’s a whole ‘nother animal entirely).
got it?
some three-legged stools are fancier than others. Here is one with “patina” – age marks that make it beautiful.
How does it work? well, my best examples are from Nepal, of course since that is where I work.
The nursing service system is organized to provide “Functional Nursing” which is to say, task-based nursing. The hospitals are not staffed to provide individualistic nursing care such as we would think of with “primary nursing” or “team-based nursing.” Oh, individualized nursing care can happen, but it is on a hit-or-miss basis.
The educational system (especially of the PCL level) teaches functional nursing. As long as the hospitals want and need functional nursing, the PCL nurses will provide it.
Functional Nursing depends on the idea that nurses do what they are told and don’t generally ask questions. Functional Nursing is a way to get the mandatory tasks done with the least number of people – in that respect functional nursing is not good or bad, it is just “is.”
which brings us to –
The role of women in the culture. In Nepal, the traditional role in involves deferring to the judgment of males, or deferring to the doctor, or deferring to who ever is “senior.” In that respect, functional nursing is elegantly matched to the culture.
If you as a foreign colleague see an opportunity to “improve things,” you need to resist the urge to jump in and implement something in one of the three legs until you have assessed the impact on the other two legs. This schema can be used to assess whether a given intervention is “sustainable.”
That’s enough for ten minutes, don’t you think? If I were to exhaust the topic, I could roll it on into about eight hours of presentation.
CCNEPal began a special project to upgrade critical care skills of nurses in 2011. Since that time we have trained 2,885 nurses and doctors to perform cardiac life support skills using scenario-based teaching, which in itself is new to Nepal.
All the props, packed up and ready to travel. CCNEPal 2016 was essentially one loooong road trip. What will we do in 2017?
2016 was lots of fun.
We conducted 24 sessions of the two-day or three-day course and gave out 715 certificates. We helped with initial training of ICU staff in some locations that were starting their very first ICU. We mostly focused on Terai (and a two-week stay in Pokhara). We taught MBBS docs from five different medical colleges. We added three sessions in Kathmandu at the end of the summer and these were terrific.
What to do in 2017?
possible dates would be June, July and August 2017. It’s all flexible until the day I buy the ticket.
This is the stuff CCNEPal uses to teach the course. Another view of all the stuff, laid out so I won’t forget something. note the “CPR manikins” deflated in upper left corner 🙂
The magic formula?
Seems to be to conduct more of these sessions. If you would like to host CCNEPal in 2017, send an email to joeniemczura@gmail.com. Wnd all the will respond by adding you to the queue, and telling you what we need in order to have a successful class ( browse the rest of this blog or else look at the FaceBook page to learn what the set up of the classroom involves. We need lots of space and a minimum of thirty participants to attend all three days).
We do not charge for this; if you are in Kathmandu Valley we request that you provide transportation. If you are outside of Kathmandu Valley, we ask that you provide fooding and lodging. We do not require a tourist hotel, just simple accommodations for one person.
There is no magic formula!
Not one that must always be applied. CCNEPal is open to suggestions as to activities for 2017. We need to always consider how to take this program and incorporate it into the professional curriculum, instead of being the add-on for those who have already graduated.
An ICU at a Teaching Hospital in Terai. Foreigners often have this fantasy that they will be in some mythic village somewhere, delivering health care to some sort of colorful ethnic group. In fact, there are modern hospitals, a system of medical and nursing education, and most of all, a collaborative approach to sharing knowledge.
I’ve been wondering about having some sort of sessions specifically for faculty of schools of nursing that want to learn how to teach this. In the B Sc curriculum, I’m told that there is a 16-hour time slot for “ACLS” – but many persons were not aware what this meant. ACLS means using this type of scenario-based teaching!
Why not have a conference to share these skills and teaching approaches with everyone? In my fantasy it would be a national conference with nursing faculty from all over Nepal!
It’s just an idea at this point, but I am putting it on a string and seeing if it will fly like a kite….. putting it in the bathtub to see if it will float ….. running it up the flagpole to see if anybody will salute….. let me know what you think…..
This is the third of a series about the two-and-a-half weeks I spent teaching critical care skills at Nobel Medical College in Biratnagar Nepal. I taught 200 nurses and MBBS students and doctors, there.
When I posted the blog about the Nepal Burn Center, my friends from Nobel sent me a reminder that they also participate in the Nepal Burn Network and collaborate with ReSurge International. In fairness, Nobel has a wide range of services including cardiac catheterization lab, and they participate in many international initiatives. But I’ll keep this short and pictorial.
This one will describe a bit more about the ICU at Nobel.
Nobel Medical College in Biratnagar has a majestic driveway, and it is a nice touch that the designers left the chautara at the beginning intact.
Resource Nurses
the two nurses in dark green are “resource nurses” – in a role similar to “in charge.” The ICU at Nobel is about 30 beds, but the physical layout is somewhat unique compared to most ICUs in Nepal. ICU is a series of rooms, with about five beds in each. each of these pods is semi-self-contained, but the nurses in the resource role float from room to room. Srijana (on the right) had taken my course at Hotel Namaskar ew years back and I was delighted to see her again. she was one of my “assistants.”
The census
one of the census boards. This is publicly viewable, which would be a no-no in USA, but still okay in Nepal.
planning
for the in-charge nurses, the day begins with report on the status of every patient
Medicine Preparation
bedside medication. they tried to stop me from taking this pic “it’s never this messy!” but I wanted to show how it’s set up. Meds are purchased by the family as ordered, using the pharmacy downstairs, and brought up to the patient’s bedside. There is also a stock medicine cart for emergency meds.
Room set up of ICU
the stock emergency med cart is against te back wall, left of center. nobody uses abbojects in Nepal, it’s all in ampules and vials. The patient on the right is being ventilated. The head of each bed is detachable. In this particular hospital, there was no distinguishing features of the room to remind you which of the six rooms you were in.
In the above, if you look closely you can see that one nurse is hanging an IV on the same pole that holds a syringe pump. Here, they have piped-in oxygen and compressed air and well as wall suction.
the inpatient pharmacy
when the doctor orders a medicine, the relative takes the scrip to the inpatient pharmacy where it is filled. always busy. these pharmacists did one quirky thing: hen they opened a carton or extra packaging, the trash went to the floor and stayed there – at times they were walking on accumulated trash six inches deep. they collected it during the slow times for disposal.
family waiting
Every patient is expected to have family available. I did not tour the ICU at night ( I realize I should have) but during the day the family waited outside ICU at the adjacent inner courtyard. it always reminds me of a bus station.
One of the families, waiting outside ICU. the sleeping pad is rolled up.
Emergency Room
panoramic shot:
Panoramic view of ER at Nobel.
I took a tour of the Emergency Room at Nobel, and made a short video. It’s a large open bay with about thirty beds, so I was interested to learn how they organized it. When a western person sees any such place, the first reaction is usually “OMG!” but there is a system that goes with it. They use the “Australian Model” –
Time passes
at the end of the time in Biratnagar, the farmers planted the entire paddy behind the guest house, as well as others. during this period, it’s like the hospital is an island in a large lake that’s only six inches deep. I left one day before the torrential rains began for monsoon 2016.
In summer 2016 I spent two weeks teaching in Biratnagar, Nepal. Though it’s the second-largest city in the Himalayan country, it’s not on tourist path. In the first part of this series I described a few things about the town. Here is what the teaching was like…..
the suite of rooms included many tables with green drapes. Nobel has just purchased a set of simulation manikins and they are developing the simulation capability. For my own sessions, I only used the equipment I brought (plus borrowing a defib and a monitor and I was careful not to let the students play with the new tools). What was under the drapes, stayed under the drapes.
panoramic view of classroom space. I asked them to bring the beds, for the small group work. the space was ideal for our training and I recommended to them to keep the beds there. in this pic, the groups are working on scenario practice, a key component of all such courses.
Lecture time
Nobel Medical College Teaching Hospital has a suite of classrooms including a very large and modern space for skills training. One end was supplied with chairs and a white board. we could jump from one configuration to another seamlessly.
;;;
from the outside, the suite of classrooms is nondescript, as a matter of fact, to get to it you needed to walk through an area under construction so it had a sort of abandoned feel. But it’s on the hospital end of the large building complex. Once you got inside it was nice. It is a fine setup for teaching
Simulation equipment, anatomically correct
okay, so when you invest money in a complete set of simulation manikins, you get the ones used to prepare nurses and doctors for Labor and Delivery. Post-partum hemorrhage is a leading cause of maternal mortality in Nepal, and a a good outcome requires a successful team response. In Nepal, a training certification effort known as “Skilled Birth Attendants” uses these. In this regard, using scenarios to drill on delivery will lead directly to better outcomes. Nobel Medical College is to be commended for their commitment to training that will benefit the region.
Simulation equipment
Effective use of the defibrillator is enhanced when you train on the device you will use in clinical practice.
on the first day of class, the MBBS students arrived in their clinical uniform which includes a necktie and a white lab coat. Here, they are reviewing use of a defibrillator. please note that the paddles are disconnected from the power source, for safety.
My contact person from the anesthesia department
my contact person was Dr. Bandana Paudel of the anesthesia department. She had trained at Nepal Medical College in Jorpati, and we both knew Dr. Gautam Bajracharya, one of my favorite docs in Nepal. For me, I love it when I meet a new person whose sense of humor matches mine. Dr Paudel is a champion of hands-on training in Nepal.
One of the defibrillators
Nihon-Kohden. Nobel has a cath lab and this is their “go-to” machine. in combination with my Pinnacle Technologies AT-35 rhythm generator, we gave students confidence in this machine.
second MBBS batch
after Day One, the Nobel College MBBS group got hip and arrived wearing the polo shirt (non-clinical) uniform, more comfortable in the heat. Al the Nobel groups shared one characteristic: they were incredibly focused. By that I mean, you could hear a pin drop when I was lecturing; they took good notes; they jumped to do the things I asked, and there was no horsing around. Some days were really hot, and they worked hard with no complaints even though everybody was sweaty. And I almost forgot: one of the MBBS batches included a subgroup of Maldivians. I gave them permission to act out the scenarios in the Maldivian language. Which they did. It was fun.
;;;
Dr Paudel maintained an anesthesia clinical schedule while the sessions took place, but I laughed when she came to help. She was the only colorful person in a sea of black-and-white. Please don’t misconstrue this comment – Dr Paudel uses the fuchsia outfit to command attention – in USA we would call this “power clothes.”
helping out my friends at Center for Medical Simulation
I gave out brochures for the classes offered by my friends at the Center for Medical Simulation in Kathmandu, Nepal’s only “Official” International Training Center for ACLS with the American Heart Association.
on teaching days I preferred not to go all the way to Guest House to eat, so I shared meals at the canteen. This was quite pleasant. I always tell people “No, I’m not teaching under a grass-roofed hut somewhere!” but, I did eat a few meals under a thatched roof.
five assistants
for each session, I recruit leaders from among the group. Here are five who served as “my assistants” for one of the nursing sessions. And Shahruk? ask me about him sometime when we meet again.
Nursing staff
Jamuna Bhatterai is Matron of Nobel Medical College Teaching Hospital and also campus chief of nursing college. she has a M Sc degree from BPKIHS and she participated in the role play. The puggri? it is not worn in this region of South Asia as a rule, but – it’s fun. And since she is “in-charge,” she also wears it as “power clothes.”
one of the group shots. I taught twentyfour sessions overall, of which six were here. Two hundred trainees at Nobel – wow. On the FaceBook page, one album shows all groups. I always stay until everyone gets a photo with me if they like.
One of the nursing sessions. The first batch of nurses were really fired up about what they learned. This created a dilemna because the ones unable to go complained. So the administrators asked if we could add a session. Which we did. They approached the training with a wonderful attitude.
acting worthy of Bollywood
As always, we did the “family counseling scenario” on day three. I’ve written extensively on this in previous blogs. The nursing groups at Nobel Medical College included excellent acting, but – the amazing thing was that they met the challenge by applying some very specific things from their own customary practice. Probably the top two of the best executed responses in the whole time I have used this scenario. I was blown away.
Training with the work team
part of the cath lab crew. Biratnagar does caths and pacing; you would have to go all the Bharatpur to find the next place in Terai (BPKIHS in Dharan also does these procedures). Over the three days they did about forty scenarios together. When they next have a critical situation in clinical, they will be a team.
Role Play scenarios
we don’t normally give the security guards much thought, until we need them. The “Gorkhali topi” is widely worn by chowkidars. Recently I read that this is considered a stereotype by members of the Gurung ethnic group. Okay. I’ll come up with better props for next year.
Felicitations
at the end of more than two weeks, we had a “felicitation” ceremony in which we acknowledged the work done by all the nurses and doctors. They gave me some nice “tokens of love.” Here I am with Mr. A.G. Singh, the Principal of Nobel Medical College. ( and Jamuna Bhatterai, the hospital Matron)
At the end of the time in Biratnagar, we had a gathering in which we memorialized the effort. This is a expression of collegiality in Nepal, and I get boxes of these “tokens of love” by the end of the summer. Call me if you need some Nepali bric-a-bracs. I hope to return to eastern Terai in future travels.
Part three of this series will show the critical care units and a bit more about the hospital itself.
In late July, 2016 I spent more than two weeks in Biratnagar, Nepal, teaching critical care skills to nurses and medical students at Nobel Medical College. This is Nepal’s second-largest city, in the eastern Terai, generally acknowledged as the center of industrial activity for the country.
As with my recent series about Janakpur, this will be more than one part. First, I’ll describe the highlights of the town, then go to the classes and finally some photos of the ICUs there.
Hotel Namaskar
This is a favorite business hotel in Biratnagar. the two restaurants on the premises were very good. out back was a party palace.
http://www.hotelnamaskar.com.np/ I stayed at Hotel Namaskar my first trip here a few years back, and on that occasion I was sponsored by “CNE Planet,” the brainchild of Raj Mehta and Dipty Subba.
Dipty is very organized and has shown initiative in continuing education for nurses in Terai. The “puggri” is not native to Nepal, but I use it as a prop for the class. It helps to get people out of their comfort zone and into the Land of Make Believe when we do complicated simulation scenarios. Naturally the headpiece includes real diamonds, rubies, emeralds and sapphires….
Hotel Namaskar is near “traffic chowk” and I never did return to it on the long 2016 trip. Traffic chowk is more pedestrian-friendly than the spot I was in, as I recall.
Videos
I didn’t shoot these, but they represent the town pretty well, in my humble opinion. You can enjoy these even without Nepali language. It’s a large sprawling city on a plain flatter than a pancake. On a good day, you can see the Himalaya.
Hamro Biratnagar (“Our Biratnagar”)
Nepali-language video
going down the street video
Biratnagar in New York Times
This city does not often receive international attention.
This one has a backstory. Biratnagar fell prey to an epidemic of Hepatitis E in 2014, a year before the earthquake, but nobody was interested from international media. Eleven hundred people contracted the illness in Biratnagar – hey! what does it take for a city to get some attention?!?!?
The New York Times seems to have re-edited this video after the 2015 quake, adding the first section based in Kathmandu, because of the threat of an epidemic; creating more interest in the Biratnagar section, where an actual epidemic happened. The miracles of modern technology allow a person of skillful means to slip the bonds of chronological time.
The Biratnagar section the NYT video includes brief glimpses of hospital scenes; yep, that’s what it looks like in a Nepal hospital!
Below is a more typical scene. Throughout Nepal this is how people get vegetables.
Geography
The east-west highway goes through Itahari. To the north is Dharan and to the south is Biratnagar. If you are in Biratnagar in summer and you need to beat the heat, go to Dharan. Here is a 24 minute travel video in Nepali that shows trip to Dharan from Biratnagar.
And now some photos I took myself.
If you arrive by bus, get off when you see this temple – the road to Nobel branches off here.
Kanchenbara is the name of the Chowk where a side road branches off to Nobel Medical College. You’ll know you’re there when you see the yellow shikhari-style temple.
Yes, look for the yellow temple, but if you are colorblind, you’ll know you are at Kanchenbara when you see this 🙂
the shop with the NCell sign is the cyber café and also does photocopying. in Kanchenbara.
If you need photocopy, get it at the cyber cafe located here.
I knew that it would be difficult to find “organic coffee” (i.e., not nescafe…) in Terai, so I brought my own supply but by this time I’d been away from Kathmandu for eight weeks. I always look for “organic coffee” and peanut butter, and – I found it for sale in Biratnagar.
simple pleasures. Nepali-grown coffee is quite good. I had been running dangerously low on the supply I brought eight weeks previous. Now – I knew I could endure anything that may come my way!
The place to obtain these is the department store at Mahendra Chowk, about 8 km south of Kanchenbara.
At Mahendra Chowk. This place has “organic coffee!” and yes, that’s a Baskin-Robbins on the right. life is grand!
Near the Chowk is the central Bajaar. On a hot day the open-air plaza is shaded by blue tarps, providing a sort of psychedic effect.
Was it hot? funny you should ask we’re talking eastern Terai in late July – yes, dear. This is the Bajaar near Mahendra Chowk.
In the vicinity of the Bajaar you can find both the Hanuman mandir and a mosque, with several adjacent shops selling Islamic supplies.
An unusual Hanuman mandir for Nepal. Usually Hanuman is outside.
Biratnagar does not have a religious focal point to rival Janaki Mandir in Janakpur, but people here are similarly devout.
The mosque at the Bajaar near Mahendra Chowk, Biratnagar Nepal.
Biratnagar has a sizeable Muslim community, with loudspeakers announcing the call to prayer at dawn.
the fun in exploring a bajaar is sometimes to guess what on earth a particular item is used for. These are clay pipes for “chillum”
Pedicabs
In Terai the pedicab business took a hit during nakibanda, the petrol “blockade.” Electric-powered jitneys, funded by business interests from India, moved in. But the pedicabs retain their charm, including colorful paintings on the stern. this depicts a Nepali kingfisher.
I stayed at the Guest House operated by the Medical College. This was quite new. Spotlessly clean and a western toilet. Here’s what my room looked like:
ithe room faced west. I loved drinking my coffee on the balcony in the morning. it was sparkly clean and the guest house staff was attentive. there was wifi.
I used the air con.
dinner at 8:30 PM around this table. the common areas at the Guest House were ample.
Dinner was at 8:30 PM, served buffet style then seating around a large table. Like other medical colleges of Terai, most of the guests were supplemental faculty from India. Dinner in Terai is always fashionably late; I have to admit I never really got used to that convention seeing as how I’m usually in bed by nine. The menu was typically “dal baat” with other thakali items. Sometimes chicken or fish also.
Kabadi
Never heard of Kabadi, https://en.wikipedia.org/wiki/Kabaddi the competitive sport, until I joined other guests waiting for dinner. They watched this for hours. who knew?
After watching the above, ask yourself what Kabadi teaches us about the national psyche of a country where this seems to be a major sport. Here is a link to the rules of Kabadi: http://www.wikihow.com/Play-Kabaddi
Breakfast wasn’t til 8 AM, too late for my tastes; we arranged a simple breakfast every day at 7 and I also got my own coffee at 0530, which was nice. People told me that some previous group of westerners had asked to relocate to some other hotel somewhere; it’s a mystery to me as to what the problem was. The staff was eager to please.
The big entertainment was to watch daily progress on the rice paddies surrounding the Guest House.
from my balcony at the Nobel Medical College Guest House. The water was six inches deep. They do *not* depend on rain to fill each paddy, it surprised me to learn about the engineering of the water – more to it than meets the eye. Also, I saw egrets. Turns out they were “Indian Pond Herons” – a new species for me.
Nursery beds
a nursery bed awaiting transplant to the large paddy. The color of newly-grown rice is dazzling. the rice-growing process provides many stories and legends and there is an annual festival when it begins.
There will be two more entries about my time in Biratnagar – one for the classes and hospital, and another for the critical care areas. stay tuned!
This past week brought the announcement of two new organizations to promote better resuscitation from cardiac arrest, worldwide. “The Global Resuscitation Alliance” and the “Resuscitation Academy.”
wow. I love an audacious goal, but – I’m a bit of a skeptic.
The two organizations were announced at #EMS2016, an international gathering of EMS personnel.
The history:
A Call to Action
On June 6-7, 2015 at the Utstein Abbey near Stavanger, Norway, 36 Emergency Medical Services (EMS) leaders, researchers, and experts from throughout the world convened to address the challenge of how to increase community cardiac arrest survival and how to achieve implementation of best practices and worthwhile programs. We call for the establishment of a Global Resuscitation Alliance in order to expand internationally the reach and utility of the Resuscitation Academy concept developed in King County, Seattle since 2008. Such a global effort will promote best practices and offer help with implementation to countless communities. A Call to Establish a Global Resuscitation Alliance1
In my Nepal sessions I always discuss the syndrome of Sudden Cardiac Death, just before I introduce MONA. I draw upon the research from Seattle, while we discuss warning signs. Turns out the people from Seattle are a driving force for this new initiative.
The Call?
from the Executive Summary of the “Call to Action” document
In 2015, twenty five years after the first Utstein meeting, 36 resuscitation leaders gathered at Utstein to solve another problem – how best to implement successful strategies in managing cardiac arrest and how to spread the lessons of best practices. This 25th Anniversary meeting is timely for several reasons:
• There is an understanding of how best practices can achieve dramatic increases in cardiac arrest survival.
• There is better science on the importance of high-performance cardiopulmonary resuscitation (HP-CPR) and Telephone-CPR (T-CPR; also known as Dispatcher-Assisted CPR (DA-CPR) and Telecommunicator CPR).
• There is the emergence of large cardiac arrest registries that provides the platform for measurement and highlights the variability in community survival rates.
• There is better understanding of EMS systems and the characteristics of high performing systems.
• There are now successful strategies to achieve programmatic implementation such as the Resuscitation Academy, which bridges the gap between science and community best practice.
• There is renewed emphasis in the proposed United Nations’ (UN) Sustainable Development Goals for 2030 to reduce deaths from non-communicable diseases including the growing problem of prehospital cardiac arrests in low and medium resourced countries.
Improving Survival from Out-of-Hospital Cardiac Arrest
• Nations with emerging economies will experience dramatic increases in ischemic heart disease and an anticipated need for pragmatic implementation of costeffective resuscitation practices.
There is a pdf download that explores the idea of best practices, and the link is:
At first I read this with enthusiasm because after all, this goes directly to the issue CCNEPal works on in Nepal. On further study, it’s not so clear. There are issues which are not addressed.
The participants were all from developed countries in the “western world” with small representation from Asia ( there were people from Singapore, hardly a low- or even middle-income country).
The participants all came from countries where there is an highly developed EMS system.
The concepts they describe apply to out-of-hospital cardiac arrest, but in the low-income countries of the world, the educational system and the service system are struggling to reach a goal of acceptable survival even with in-hospital cardiac arrests.
Finally, the sponsoring organizations have a vested interest in promoting only those initiatives that already fit in the proprietary box. For example, in order for a training course to receive approval by the American Heart Association, it must meet the same criteria when taught in Timbuktu (or Kathmandu!) that it would if taught in the USA. If the goal is widespread dissemination of resuscitation skills, this is simply not practical and it smacks of “cultural imperialism.”
From my own experience?
Here is my feedback to this initiative. The scope of need is vastly greater than can be met by using the approach now in favor with the developed countries. Considerable “ramping up” is needed.
For the “official” AHA ACLS course, equipment costing about $25,000 is needed. Few in Nepal can afford this investment.
Only the approved DVD may be used for the didactic component, and all discussions, including the debriefing must be done in English (or Spanish is also allowed).
This is simply ridiculous, and has been generally rejected. Obviously a doctor or nurse can be an excellent ACLS team member or leader even if they speak no English whatsoever – the physiology is the same regardless of the language spoken by the person who is delivering the resuscitation.
Next, such skills as airway management using a bag-valve-mask, reading an ecg, or using a defibrillator, are not presently taught in medical colleges or nursing schools in low income countries.
Finally, no one country or language group should “own” the knowledge. The scientific studies on which the protocols are based, belongs to all of us, no matter where we reside on the planet.
Companions
I hate to sound like I’m only ranting, so here are some ideas:
Why not a companion set of goals for “Improving In-Hospital Response To Cardiac Arrest?” especially in low income countries.
What about convening experts in this area from Africa, and/or South Asia, and/or other regions, to discuss ways to address this based on a non-Eurocentric approach?
And finally, for Nepal – facing an epidemic of smoking-related cardiovascular disease. How can Nepal tap into this expertise to develop a sustainable system combatting this problem?
Summary
people in Nepal are working on these issues, piecemeal. Somehow Nepal gets left out of the discussion when trying to develop a “Global Alliance” – hey, Nepal is on the same globe as USA is……
And today? part three describes JHCRC – Janiki Health Care and Research Center.
Raman Mishra, MD
Dr. Raman Mishra was my main contact in Janakpur. He is an internist, trained in India though Janapur is his home town. He is working in an impoverished area of Nepal and his vision is to improve health outcomes. We generally met each day after work to chat about the best way to do ICU and how the training was going. I love a “college bull session” when we discuss how to improve critical care and prevent excess deaths.
entourage
I joined Dr. Mishra on rounds several times. He generally was accompanied by an entourage of MBBS students, Medical Officers, interns and hangers-on. Rounds start in ER, that’s where the critical patients go since the ICU is not presently opened.
Dr. Mishra seemed to be seeing several dozen inpatients each day as well as maintaining an outpatient schedule. In order to accomplish this feat, he heads a team of interns and Medical Officers. This is an important point: JHCRC is in a region that’s low on the development index ( even within the country of Nepal) but there is a system, a hierarchy, and daily followthrough.
auscultation. Dr. Mishra always includes the family on every discussion, twice a day.
JHCRC does have it’s own web page: http://janakihealthcare.com/
They have an active pediatric service and Neonatal ICU.
Administrative duties
I was committed to exactly two weeks in Janakpur, and no more. Here Dr. Mishra is going over the list of attendees for JHCRC batch one. We were going to do an MBBS batch later in the week, but nurses felt “left out” from the first batch and complained bitterly, so we adjusted the schedule and poof! the second batch at JHCRC was for nurses and H.A.s
JHCRC – the complex of buildings
The one-and-only gate to JHCRC. As readers of this blog know, focus of my work in Nepal is to mitigate violence against health care workers. Here is a built-in security feature.
the outside walls….
the east side of JHCRC abuts one of the ponds. sort of a moat, actually…..
at night –
inside the courtyard, at night, the ER is the door to the right.
and in the daytime
all services at JHCRC are arranged around the inner courtyard.
my room –
JHCRC has two guest rooms on site, in an out-of-the-way spot, for visiting doctors. I could have stayed in a hotel, but I preferred to be closer to where the activity was. The room had air con. I confess I needed it after each full day of teaching ( the classroom at JMC had fans but no air con and I was beat!)
The kitchen
throughout the Terai, dinner is usually at 8 or 9 PM. I don’t like to wait that long, and I also like to putter around and make my own coffee early in the morning so they gave me my own key. There was also a refrigerator.
mosquito netting
There weren’t many mosquitos and I also was taking prophylaxis, but – since it was there I slept under it. The bedroom also had air con… teaching during the day in the heat was exhausting, so I admit I used the air con every evening while I rehydrated.
dormitory for patients from distant areas
every few weeks, an ophthalmic surgeon comes to do a flurry of cataract surgery. JHCRC has a small dorm to house the recipients for a few days – so they can be accessible to followup despite living a distance away. I thought this was a nice touch.
the New ICU under construction
The new ICU at JHCRC. during the past few years, JHCRC has been the “go-to” with high occupancy rates. It was finally time to invest in ICU construction. They were adding the finishing touches while we were there.
the JHCRC courtyard
participants in CCNEPal training
the first session of JHCRC. this was a smaller batch than usual for me, due to space considerations. They worked hard and helped each other.
JHCRC leadership
The CEO of JHCRC is Dr. Surendra Yadav, MD. He led the setup of the system of health posts that are part of JHCRC, funneling patients from the rural areas to the hospital when needed.
Dr Baghat
Dr Sarban Kumar Bhagat of JHCRC was the on-site administrator. Here he’s talking with the class about the certificate.
another view of soon-to-be ICU
a panoramic shot of the ICU space while it was set up for training purposes. piped in oxygen and suction; air con; and big fans overhead.
The second batch
the second JHCRC batch, in the soon-to-be-opened ICU. In Nepal, men aren’t allowed to attend nursing school – they attend “Health Assistant” training instead.
time to move to next location, but not until a few formalities….
at the end of two busy weeks, I got “felicited” – which of course, I love.
Token of Love
My”Token of Love” from Janakpur was a silk screen done in Maithili style (note the iconic eyes) depicting a wedding. I shall cherish this!
In Summary
Janakpur is the hub of a fascinating region of Nepal, not on the beaten track for western tourists. There are other hospitals besides JMC TH and JHCRC, including a large and busy zonal hospital. But without JMC and JHCRC they would not be producing health manpower likely to stay in the region. Janaki Medical College hosts many doctors from India; but very few from western countries For teaching purposes they are interested to host more and to participate in international exchange.
There will be a part 3 to describe Janaki Health Care and Research Center – JHCRC.
This one is about Janaki Medical College Teaching Hospital – city branch. JMC TH.
When I go to Nepal I always start with a blank slate. I know I’ll be invited here or there. This time I wanted to make a swing through the Terai. Since my bus accident last year, I wanted to minimize bus travel.
I wanted to go to Janakpur, since it was halfway between Bharatpur and Biratnagar. So when I got an invite out of the blue, I said yes.
Janakpur and their travails
For those not in the know, Janakpur has a medical college and they had some turmoil two or three years ago. The medical college operated two teaching hospitals – one in town and one outside the city near the campus. The one in town got closed for seventeen months. The college replaced all their managers. The college was also on probation from the Nepal Medical Council. All of this is public knowledge.
Among the new leaders brought in was a doctor originally from Janakpur who had been practicing in India. Dr Raman Mishra attended medical college in Varanasi and was a member of a medical practice in Chardigarh. He returned home. His practice includes both Janiki Medical College Teach Hospital (JMCTH) and Janiki Health Care and Research Center (JHCRC). Because JMCTH had just re-opened after seventeen months, he was re-establishing the ICU there. At JHCRC, he wanted to open a specific ICU, because there was none and ICU-level patients were being served in the ER.
Dr Mishra found this blog via websearch.
Next thing you know, Janakpur was on the schedule!
JMC TH has reopened and they are being renovated. They have not yet recaptured their previous level of activity. JMC has another hospital on the outskirts of town as well. I did not visit that one.
I did five sessions there – two at JMCTH and three at JHCRC.
Here’s a photo of JMCTH ICU:
Now, an interesting thing about Janakpur was, there were already a couple of nurses who’d previously taken my three-days’ course when I taught in Bharatpur a couple of years ago. Also, the enrollees at the first session included B Sc students from the JMCTH College of Nursing, along with their faculty members.
Nursing faculty of the JMC College of Nursing.
Binu Shah
Turns out that unbeknownst to Dr. Mishra or myself, one of the JMCTH nursing faculty had gotten her M Sc in cardiovascular nursing from the UK. Binu Shah was very knowledgeable resource, and I soon asked her to help with the teaching. I love it when this happens!
Binu Shah of the JMC TH college of nursing faculty, at the blackboard. It turns out that Janakpur has more knowledgeable persons in the workforce, than we thought. In this respect I was effective at calling them out of the woodwork and getting them introduced to each other. Hey – if it works, I will try it! Among other things, Binu helped translate the more difficult concepts into the local language. My motto is “you can be great at this even if you speak no English” – and for the record, I personally speak *no* Maithili. Binu made these sessions a success!
The JMC TH ICU nursing staff was enthusiastic and came early to make sure they mastered the defibrillator.
JMC TH owns two defibrillators. The staff was diligent in learning the course content. Here is my AT-34 rhythm generator attached. I teach three methods of ecg – the six rhythms, the six steps, and the eyeball method. The generator is a fun toy.
The groups
The groups included a couple of Medical Officers and some “Health Assistants” from the Emergency Room. (Health Assistant is a person with a three-year PCL diploma). In this region of Nepal, the main language is Maithili, on par with Nepali and Hindi.
Classroom setup at JMC TH. we used a vacant patient care area. the course jumps from lecture to small-group practice, so the space was nice to have.
The sessions
Binu Shah helping explain concepts of cardiac arrest at JMC TH. She is a resource for that region of Nepal and I told her she should be teaching this class in the Janakpur region.
Groups
JMC TH nursing students. These guys will be the nucleus of future critical care nursing practice in Janakpur. please note that the paddles are disconnected from their power source, for practice purposes.
and
JMC Th B Sc students in the second batch at JMC TH. They wear a different uniform than the PCL nursing students. Here, they practice the eyeball method of ecg.
One of the JMC TH batches for CCNEPal in summer 2016. Shahruk Khan has a prominent role in each class….
I spent the summer of 2016 teaching the CCNEPal course in Nepal, mostly in Terai. I was invited to teach in Janakpur, in eastern Terai for two weeks. It turned out to be a highlight of the summer. I am proud of what I was able to help them accomplish there. I am writing two blogs about Janakpur. The first one will just tell about the town and the second will focus on the medical scene there.
The Janiki Mandir celebrates the Ramayana, a famous Vedic epic from ancient times.
Janakpur is in an out-of-the-way section of Nepal, and it is a miniature version of Benares in many ways. The main language is Maithili, not Nepali or Hindi.
Hanuman figures in the tale of Ram and Sita, and so there is a temple for him. The woman in the picture offers puja at a bo tree on the ground of the Hanuman Mandir
The Town
This is still in progress but I thought I would publish the rough version.
To learn about the town, there still is no better place to start than the BBC series on railways in India, that features the last railway in Nepal:
The tracks are being completely redone, and the railway station is not serving any travelers. I was told that during monsoon, the only way to get to the villages along the rail line is by the train – none of the roads are passable. People living there need to have all their supplies in, before the rain starts.
Next is a fourteen-minute English-language travelogue touting a packaged tour for Hindu pilgrims. (not my video, obviously)
Lex
Here is another English-language video, four minutes. The narrator decided to highlight parts of Nepal that were *not* Pokhara or Chitwan. Bravo!
Here is a ten-minute video that shows daily life in a village. It’s in Maithili; Note the wattle-and-daub construction – typical of this region of Nepal.
Summer monsoon 2016
aerial view of Janakpur’s summer monsoon flood, August 2016. From Republika.
I left the eastern Terai one day before the serious rains started. Above is an aerial view of the floods as they impacted Janakpur. This is no joke!
The bus stop
yes folks, this is how I roll in Terai. This one was going to Itahari, from Itahari I transferred to the Biratnagar bus. On the Biratnagar bus I received a marriage proposal. I declined.
the main truck route through Janakpur. You’ll know you have arrived when you see the fanciful gateway. directly east of the gateway about five blocks, is the Janaki Mandir. the highway itself at this point, is not scenic.
helpful guy at the ticket shop
There are few English speakers likely to be found at the bus stop. Look for this shop on the western side of the road, and this guy. He speaks English and is very friendly and helpful.
on the west side of the highway this guy in the white t-shirt speaks English and was friendly.
here is a better shot of the guy, his name is Ram.
Agriculture activity
out front of the JHCRC hospital one morning. they are taking the bamboo to a construction site.
One Planet
the local dalits keep pigs and eat pork – something no Hindu or Muslim would do. A squad of pigs roams the town. In public health, there is a movement known as “One Planet” which acknowledges that when humans live in close proximity to animals, both domestic and wild, the health of all must be considered, not just homo sapiens
Cyber Cafe
wi fi was available at the hospital, but I found the one and only cyber café in town. reasonable rates. not far from Janiki Mandir, on the road to the zonal hospital.
I stayed on the premises of the host hospital, but most foreigners go to one particular hotel downtown:
my hosts offered to put me up here, it’s where most westerners stay. But I was fine with the accommodations at JHCRC. I never did eat at this restaurant either.
While we are at it, in the vicinity of the hotel is the one and only “Department Store” of Janakpur. I always check to see if they have a) “organic coffee” and b) peanut butter. They did not stock either item. They did carry many other western items though.
the main drag of Janakpur goes from Ganga Taal to the railway station. at the back of this alleyway is the department store. They did not yet carry “organic coffee”
inside the department store n the main drag of Janakpur
Saturday evening Hindu worship at Ganga Taal. This is popular. There are thirty lakes in the city limits. On the far of this one is the funeral ghats of the town.
Janaki Mandir
in front of the Mandir is a plaza. They were televising a tent meeting the week I was there.
The centerpiece of the town is the Janaki Mandir. Here’s a short video showing how it’s decorated with lights:
A sacred cow
my cousin read this blog and she asked as to the significance of the pink cow. My reply? *what* pink cow? I don’t see a pink cow!”
Puja Supplies
a portable shop for textile puja items.
More puja supplies
these are inexpensive.a staple of home puja altars in South Asia.
and more
pujas supplies on the plaza of Janiki Mandir
Because of Ram and Sita, a love story, the temple is popular for weddings, and something that astounded me was the number of processions, usually at night, and always with – a brass band. Sometimes two or three parades converged on the plaza at the same time – glorious chaos!
The Ram mandir is a stone’s throw away. The backside of the Ram Mandir is under construction:
the backside of the Ram Mandir was under construction. There is an interior courtyard for Kali at this site, I’m told it’s quite a scene during Dasain. to the right, out of the picture, is a lassi shop and pan shop, well worth the visit.
Front of the Rama Mandir
much more imposing, don’t you think?
the main entrance to the Rama Mandir. Much grander than the back!
Dahi
Dahi is yogurt. I eat a lot of it as a preventive measure, but none of the shops carried any.
here is where reading devanagari comes in handy. I would have walked past if I had not been able to read the sign advertising “dahi” – fresh yogurt. This shop is near the mandir, headed towrd the water storage tower.
I had some, and it was creamy and wonderful. I thought it rivaled the yogurt of Bhaktapur.
I asked to take a photo and the shopkeeper got a new vat of yogurt out of the fridge. the yogurt here is every bit as good as the fabled yogurt of Bhaktapur!
Lassi
I found the lassi place on my own accord, then I was told this is considered to be the best in the district. Mitho 6! The guy behind the steel counter is the pan saudji – i.e., betel nut. In my experience, betel nut is more popular in Terai.
Leaves for Pan
Basket of leaves in the marketplace, arranged just so. I learned that this is how the pan sellers like them. When you buy pan, there is a ritual of how it is prepared at point of sale.
a panoramic shot of the front of the temple, showing the plaza.
I was in Janakpur to teach critical care skills, and taught five sessions with about 125 participants. (the pic shows just one of the groups…) I’ll do a separate blog on the actual teaching. Together we worked to strengthen critical care practice in a town serving about 600,000 people.
My”token of Love” from Janakpur was a silk screen done in Maithili style (note the iconic eyes) depicting a wedding. I shall cherish this!
The piece includes a description of the incident, as well as a graphic photo ( not re-published here). It also gives an update on the prevalence of burn injuries in Nepal, including some statistics, such as the fact that in 2018 there were 56,000 burn injuries in the country. On Facebook, somebody posted this commentary:
ना बेटी को पढ़ाई जाती है, ना बेटी को बचाई जाति है , बेटियाँ तो सिर्फ जैसे तैसे पैदा हो जाति है। पहले गर्भ मे हत्या की प्रयास होती, बच गइ तो बचपन मे लापरवाही करके मारने प्रयास होती है, फीर भी बचाई तो कोई पापीलोग रेप करके उनकी हत्या कर देता, अगर ईस से भी बच गई तो भिखारी लोग दहेज के लालच मे उसे मार देते। और इन सब से बच गइ तो भी कुछ पापी पति और कुछ क्रुर औरत (सासु) ही उनकी हत्या कर देती। फीर प्रदेश सरकार कहती है बेटी पढावो, बेटी बचावों।
अरे बहुत होगया सरकारी नाटक, कुछ कर सकते हो, तो कड़ी कानुन बनावो और ऐसे जानवरों का सफ़ाया करो! प्रदेश की राजधानी, धनुषा जिल्ला और उसके आसपास ५ औरतें मारे गइ है और वो भी पिछले १२ महिना नही, पिछले १२ हफ़्ते भी नही, पिछले १२ दिनों मे।
पिछले साल बहुत स्कुल भर्ना की नाटक किया सरकार ने, कहा गये आज तुमलोग? बेटी को तुम पढ़ा तो सक्ते नही, कम से कम यिनहे पापीयो से बचावों।
Translation of above:
Neither the daughter is taught, nor the daughter save the caste, the daughters are just like the one who is born. In the first pregnancy, there was an attempt to murder, if you survived, then there is an attempt to kill in the childhood, even if the fear is saved, some sinners would have raped and killed them, if they were saved from this, then the beggars would have killed him in the greed of dowry. Even if i escaped from all of these, some sinner husband and some cruel woman (Mother-in-law) would have killed them. Fior State government says daughter teach, daughter save.
Hey, a lot of government drama, if you can do something, then make a strong law and destroy such animals! The Capital of the state, DHANUSHA DISTRICT AND 5 women around it have been killed and they are not even the last 12 months, not even the last 12 weeks, in the last 12 days.
The government has played a lot of school admission in the last year, where are you today? You can not read the daughter, but at least you can save the sinner from this.
Don’t tell me that this never happens.
April 2018 Update: six-minute CNN video about the Burn Center in Kirtipur
March 12 2018 update: Today’s Nepal news is a plane that veered off the runway while landing and burst into flames. Two dozen victims survived and were brought to hospitals in Kathmandu. I am sending the victims good karma and also praying for God to guide the hands of the doctors and nurses. In the meantime, in such an accident there is a high proportion of burn injuries. And so, I am re-posting this blog entry for people who wish to learn more about the health care system of Nepal.
In January 2016, I wrote a piece about burn care on my other blog, titled “Bride Burning” in Nepal and Burn Injuries http://wp.me/p3b3md-e1
My first book told the story of my first trip to Nepal. I worked with burn victims in 2007. Half the book is devoted to that experience. Burn injury is a big problem in Low Income Countries.
This summer in Nepal I had the serendipitous chance to teach my course at Kirtipur Hospital, home of the Nepal Burn Center.
The hospital building is relatively new and still under construction. It serves a dual purpose, both as burn center and community hospital for the town.
Kirtipur is an ancient town in the Kathmandu valley, home of a large campus of T.U., and southwest of the center of the city, outside the ring road.
And below the photo is a video from a few years back that features Dr Shankar Rai, a reconstructive surgeon.
The fabric of Kathmandu’s bus system shows a wrinkle near Kirtipur since it takes two changes to get up the hill. This is one of the ad hoc bus parks.
The hospital is presently administered by Kathmandu Model Hospital. They freed up thirty staff to attend the CCNEPal three-day course.
the participants were a cross-section of hospital departments. Here, we’re about to do a demo of one of the scenarios of the course.
There is a wonderful nurse from Australia who is working through PHECT, named Tina Bryce McKay.
Tina Bryce McKay is a nurse from Australia who works at Kirtipur via PHECT. Earlier in the summer she came to Pokhara to help me.
I did not think i would teach in Kathmandu Valley, but when the schedule changed and I got some time, Tina got me the invite to train staff at Kirtipur.
Tina ( blue bandana) works to elevate the standards of staff training. Here she is, guiding a nurse through ecg analysis. Quite a bit of the class is devoted to elementary ecg and how to incorporate it into overall assessment. Any person who says ecg is not a cornerstone of critical care, does not know what they are talking about.
They gave me a tour of the place.
panoramic view of post-surgery ward during morning rounds. the layout is a large open space with low walls. The screen is used when dressings are change during rounds.
close-up of dressing cart
minor wounds will be examined at bedside and major ones go to “Theatre”
and another view:
Family involvement
Here is the waiting area outside the HDU, where patients are admitted when they have the most extensive burns. In Nepal, the family is expected to be nearby. In many cases, they donate skin to the victim.
just outside HDU. the gowns are used when visiting their loved one.
In the area where the HDU is, the Operating Theatre has a room designated specifically for grafting and debridement.
preparing for a debridement procedure. this would be done under light anesthesia to decrease the pain involved.
The HDU is a highly specialized Intensive Care Unit. When extensive burns occur, the victim inhales hot gas and can burn the upper airway. Inhalation burns are extremely serious.
panoramic view of HDU at Kirtipur. There were six burn victims that day. All required ventilatory support. All had suffered burns of greater than 60%
The percent of burns is an important point. For years it has been an axiom in Nepal that >60% burns is not survivable.
The “HDU” at Kirtipur is the most active critical care unit for burn victims in Nepal.
The physical plant of the hospital is only part of the story. In this case, Dr Rai – the main doctor behind the establishment of the hospital – is also a faculty member of NAMS, the National Academy for Medical Science, the oldest site for Post-Graduate Medical Education in Nepal. Along with other surgeons from NAMS, they have built a nationwide network to educate for best practices in burn care. Course have been held in many regions of Nepal, and local educators have been trained. They work with Nepal Burn Society; with Interplast; and with ReSurge International.
Here is a video from only two years ago that updates Dr Rai since the earlier one above. It was made just as Nepal Burn Center was being built.
Another piece of the medical system needed for effective burn treatment is to have a skin donor bank. – http://setopati.net/society/1073/
The hospital at Kirtipur serves a critical need in Nepal to upgrade the level of burn care. Their efforts go beyond the construction of a physical building – they are also creating a nationwide network for burn education and care. They partner with international NGOs to advance the practice. Burn care is intense, and it’s inevitable that they will have staff turnover. They need to continue to train their staff, and I think they could benefit from partnering with NGOs that will send future nursing specialists in Burn ICU.
My own efforts to educate nurses and doctors in advanced life support have paralleled the approach adopted by the Nepal Burn Society, I am impressed by their success.
Original goal for summer 2016 was to teach as many sessions as possible, focus on areas of Nepal outside of Kathmandu Valley, while yet minimizing bus travel.
Each session is two or three days in length, and consists of a variety of short lectures and discussion punctuated by “megacode” – simulated critical situations requiring a team response and return demonstration of specific scenarios. Here is an example of how the group breaks into “megacode” activities:
(above video shows how the class divides into five groups for practice of scenarios)
At each location, I was humbled by the hospitality, support and enthusiasm of my hosts and the students.
Dr Umid Shrestha of Pokhara is a faculty member of Manipal College of Medicine and a supporter of upgrading the nurses role in critical care in Nepal. He has supported CCNEPal from day one.
The means of deciding where to go was the same as in in past years. I announce my dates of availability on FaceBook and people contact me. I see what can fit the schedule. I email individual places that were on the waitlist of previous years to remind them I’m coming back. And it happens. It was amazing to see that based on word-of-mouth, I could refill the schedule at a moment’s notice when something changed. Every session but one was full – (there was one session for just five MBBS students in Biratnagar that fell on Eid).
Please note: If I return in 2017 I will again use FaceBook to announce the dates.
The list of venues was:
Pokhara:
Paschimanchal Community Hospital
Tina Byrnes of “Phect” joined me in Pokhara to see my ing methods. She is a nurse frm OZ now working at Nepal Burn Center and I returned the favor by collaborating on a session later in the summer.
Charak Community Hospital
Bharatpur:
College of Medical Sciences
The College of Medical Sciences Teaching Hospital in Bharatpur operates one of the busiest Emergency Rooms in Nepal. They first hosted me in 2011.
Pushpanjali Community Hospital
Janakpur
Janaki Medical College Teaching Hospital ((JMCTH)
Janaki Mandir is a major Hindu site in Nepal. the BBC documentary “Last Train in Nepal” was filmed here.
Janaki Health Care Center and Research Center (JHCRC)
CC
Here is a BBC documentary from a few years back that portrays a fascinating view of life in this region of Nepal.
JHCRC was my host in Janakpur. They were at 100% occupancy while I was there.
Dr Raman Mishra (L) was my main contact in Janakpur. He was educated in Varanasi and practiced in Chandigarh India prior to returning home to Janakpur last year. In this photo, he is beginning the day with rounds accompanied by his entourage.
Biratnagar
Nobel Medical College Teaching Hospital
Nobel Medical College is a major complex and they provide comprehensive services including a cath lab
Nobel has committed to the use on education, investing in equipment and a training hall.
the main training hall at Nobel Medical College
Bharatpur
Chitwan Medical College
Kathmandu
Bir Hospital School of Nursing,
Norvic International Hospital, and
Nepal Burn and Cleft Palate Center in Kirtipur
The “HDU” at Kirtipur is the most active critical car unit for burn victims in Nepal.
Total number of certificates awarded:
715 – including nurses, MBBS, Medical Officers, Health Assistants, and Nursing students.
Number of sessions:
24. Most weeks I worked six days per week.
Travel days
six. Instead of staying in Kathmandu and going out-and-back, out-and-back, I did a circuit.The longest was from Biratnagar to Bharatpur.
Cumulative totals:
from previous years, 2170 participants in 70 sessions.
2170 + 715 = 2,885 participants.
70 = 24 = 94 sessions
Discussion
The fundamental challenge of acute care in Nepal right now is that the hospitals are installing critical care units but the nurses and junior doctors are not trained to conduct their activities at the skill level required.
Nurses do not read ecg. Nurses have a superficial knowledge of equipment such as bag-Valve-Mask devices or ventilators. The primary system of nursing education teaches “Functional Nursing” which is the antithesis of the critical thinking required to assess and evaluate nursing care to a critically ill person.
Junior doctors, likewise, are not given any kind of formal ecg class, nor do they do BLS or ACLS training. During the internship year they may be conducting the team response to a cardiac arrest but have never been trained as to the protocols in any practical way.
Overall cultural factors tend to work against interdisciplinary collaboration due to the perceived role of women.
This continues to be a gap in health professions education in Nepal. The overall education system is theory-based and there is no transition to the practical-based focus exemplified by BLS, ACLS and the like.
Future Directions
CCNEPal will continue to advocate for inclusion of BLS and ACLS-type training in undergraduate nursing schools, including PCL programs.
CCNEPal will endeavor when possible, to introduce these methods to faculty as well as critical practitioners.
CCNEPal will identify leaders who can teach this themselves.
CCNEPal will introduce the teaching methods and skills to as many medical colleges in Nepal as possible, and advocate for course placement in 4th year of MBBS or at start of Internship year after MBBS.
quite a bit of the class is devoted to elementary ecg and how to incorporate it into overall assessment. Any person who says ecg is not a cornerstone of critical care, does not know what they are talking about.
CCNEPal will continue to share information about Nepal with medical and nursing schools in the west as well as with individual persons wishing to collaborate with Nepali health care organizations.
this is for my USA readers. Most of the time I comment on events here in Nepal it’s directed to a Nepali audience. Not this time.
In USA these days the wish to include a Global Health experience into education is stronger than ever. For medicine, nursing, public health, and other specialties, the college or University graduate programs are testing the waters for clinical placements of various kinds. Nepal has always been an adventuresome choice for brave souls, and Nepal has a mystique about it that beckons.
Expanding the menu
The vast majority of North Americans go to just one or two locales in Nepal for an elective, and these are getting crowded. The magic gets diluted when it becomes a stop on the international trail. For example, one of the more popular places is now hosting up to a hundred foreigners at any given time. This changes the nature of the experience. A related question is “With twenty medical colleges in Nepal, why is it that only two or three become the hosts of the foreigners?”
Serving as a resource
At the spring 2016 meeting of the Consortium of Universities for Global Health, I met many people who asked if I’d share contact information at all the places I go, and give advice as to what medical services were offered. So I plan to compile a sort of offbeat guidebook to the hospitals and schools with which I interface.
I’ll include photos, a description of the geographical location, pics of the buildings, and contact information of key people at each place.
Travel agency?
Um, no. I’m not a booking agency. I think there are many different levels in which a professional person can participate in global health. My audience for this would be people with bonafide credentials that wish to gain perspective. This is not ” trekking with toothbrushes”nor is it volunteering at an orphanage or teaching English to Tibetan exiles. Those are worthwhile for some people, but not related to what I do when I am here.
So be on the lookout. If you have questions, send me an email.
I’m back in Bharatpur, where I was a month ago. The return bus ride through eastern Terai was wonderful – like riding through The Shire.
Statistics to date:
As of today I taught 19 sessions, with 560 certificates awarded. The present plan is to teach five more sessions, with possibly 150 more certificates – if that works out it will mean I trained 710 nurses, doctors and others, this summer. On the FB page, I made a photo album that consists of one group picture for each batch.
It is a large number of people, and the goal has been to introduce the idea of ACLS as widely as possible.
The schedule?
July 24th, 25th, and 26th – Chitwan Medical College staff nurses.
July 27th, 28th and 29th – Chitwan Medical College B Sc Nursing students
July 30th – travel to Kathmandu via bus. should be the final bus trip of summer 2016. Hooray!
July 31st, Aug 1st Aug 2nd – BN students at a school of nursing in Kathmandu.
August 3rd, 4th, 5th – Norvic Hospital, Thapathali
August 6th, 7th and 8th – possibly a hospital in southern Kathmandu Valley.
August 11th – return to USA.
It’s been a productive summer and I have brought the info to new places. I previously taught 2,170 people, the grand total will now bump up to 2,880 if the plan holds up. Many thanks to all who made it possible.
In Charikot, Dolkha district, there was an “incident.” I do not pretend to know the details, but one pertinent feature was publishing a videotape of the doctors involved, apologizing for what happened. Fortunately, these particular doctors did not get “thrashed” – but the video had the effect of making the incident very public and underlining the threat faced by young doctors in Nepal as they work with limited resources in rural areas.
Original story (written long before the “Charikot Incident”)
When a patient dies, the doctor is often blamed, and the family is angry. Thrashing the doctor is is a problem throughout Nepal. I made this list for my most recent sessions of Critical Care Class. The reality is, we are all going to die, and when we do, there is nobody to “blame.” It is not the doctors fault.
Communication is the key
Effective resuscitation more than just the ecg, BLS and drug protocols. The leader of the team must manage the interactions with patient party, and also with administration and police if things do not go well.
The Leader of the resuscitation team must recognize that the team is not just the other doctors and nurses, but also the guards and sometimes the police. It is not enough to only focus on resuscitation. Also, in previous blogs I have given link to checklist for secure building.
1) Goals The goals of resuscitation are always:
a) conduct the most effective resuscitation effort possible,
b) allow family to express emotion, and
c) keep all parties safe from harm.
2) Weapons if any patient party shows a weapon, run away. You are never being asked to sacrifice your own life for doing this work.
3) Access limit access to emergency room or ICU asap when critical situation develops. All exits and entrances must be guarded or secured.
4) Security Guards communicate with chowkidars. This is two-way. Chowkidars serve as eyes and ears beyond the ER door. If patient party outside is upset, they alert staff. If staff is having problem, guards are notified. If problem develops, chowkidar sends for extra help. If ER doctor directs doors to be shut, immediate limitation of traffic must take place.
5) Police pre-enter phone numbers of administrators and prahari into all smart phones. If a situation gets out of hand you do not want to be looking up the number. For that matter, invite the local police to the ER on a quiet day so you will know each other.
6) Counseling send staff person to sit with anxious relatives. Staff person assesses education level and directs teaching to most educated person present.
7) Chairs give patient party opportunity to sit. (more difficult to get physical).
8) period of respect after death if death occurs, ALWAYS wait fifteen minutes before allowing family to view the body so that remains will no longer be “twitching” – this is very upsetting and confusing to many persons.
9) mutual support doctor brings a nurse and chowkidars when counseling patient party.
10) Tone of voice pay strict attention to tone of voice of staff at all times. Apply principles of “de-escalation” whenever tone starts to escalate.
This blog has given ample advice on this subject, browse past entries to learn more.
I loved meeting all the people there. Dr. Umid Shrestha of Paschimanchal Community Hospital and Matron Sushila Neupane of Charak Memorial Hospital were wonderful hosts. I thank them. They are visionaries for the future of critical care in Pokhara.
I gained much appreciation for the level of skill to be found among the interns and medical officers from Manipal College of Medicine.
I think the ICU at Charak Hospital is every bit as well-organized as any ICU in the Kathmandu Valley. An ICU is measured by the skill of the nurses, not by the equipment list.
Students in the nursing sessions came from PCH; Fishtail Hospital; Fewa City Hospital; Western Regional Hospital; and Gandaki Medical College as well as from Baglung, Damauli, and Gorkha. I was joined for one session by Tina Byrnes, RN from Sydney who is conducting a nursing project in Kirtipur under the aegis of PHECT, an Ozzie quasi-governmental entity. I think I gave her a few ideas.
I did not previously know there was a “New Road” in Pokhara.
Bharatpur, College of Medical Sciences
June 4th was a bus trip to Bharatpur for the next leg of the journey. I’m trying to minimize bus travel.
I got to the tourist bus station okay and used the toilet there. Normally I wouldn’t add such a detail, but the electricity was off and the toilet was pitch black dark. Not even one photon. Ever try to use an unfamiliar bathroom in the dark? I didn’t want to use my smartphone flashlight for fear of dropping it in ” the hole”. In the process of getting my trousers back up, my wallet slipped from my pants pocket. I ran back for it when I noticed it missing, almost left it behind. I do a lot of “check twice, you’re not coming back here again” when I travel, glad to have developed the habit of patting myself down.
From Pokhara to Mugling the road travels through a scenic region that evokes “The Shire.” Looking out the bus window was a travelog of village life in the hills – verdant fields, people tending to tasks of daily life. The road between Mugling and Narayangarh was a mess, due to a widening project. Many stretches of one-lane road. The drivers were patient with each other. It will be great when it’s done. Just not now. The Nepali method of road widening seems to always start with demolishing the previous road. This is the road that hangs on the steep side of a river gorge. There are places where it seems like the engineers just flung it up there to see if it would stick.
We’ll have three sessions of the course here at CMS.
June 5, 6, 7 – 4th-year B Sc nursing students. (thirty)
June 8, 9, – MBBS/interns. (twenty)
June 12, 13, 14 – 3rd-year B Sc nursing students. (thirty)
My contact person here is Mrs. Sita Parajuli, Matron of the Hospital and Campus Chief. Sita Ma’am was in Tansen for many years, so even before I met her here in 2011 we shared many mutual friends. Sita Ma’am has advanced nursing in the Terai. Due to the education system here, CMS faces turnover among the nursing staff. Young PCL graduates stay two years then go for their BN degree (this system is being changed because of this very problem). Sita is always growing the leaders and the staff.
June 15th, 16th and 17th are open dates. I’ve been asked to work with one of the small hospitals here, this is not confirmed. If I do, I’ll post it for possible students to join, who may be otherwise unafilliated.
Janakpur?
June 18th I leave for Janakpur, home to the famous temple. I am told they are starting up an ICU in that city. The time is just flying by.
Kathmandu?
I’ve gotten inquiries about Kathmandu sessions. There are none planned. I’ve spent ample time in Kathmandu in the past. About 800 nurses and doctors there got my training. Sure, there is demand for more, but Kathmandu has many people who could be teaching this.
A comment about mission of CCNEPal
CCNEPal’s goal is to promote critical care skills using a training method exemplified by the BLS and ACLS courses of the American Heart Association (AHA) in USA. We are emphatically *not* part of AHA, and this course does *not* lead to AHA certification. Due to AHA’s impeccable and authoritative scientific research about resuscitation, we do teach the AHA standard when we can – adapted to the needs of Nepal. Participants learn in Nepali language. You do not need to be expert English speaker to benefit from this training.
It has been obvious from the beginning that we need to teach “what ACLS is” before we can teach how to do it. That is why we offer our sessions to the largest number of nurses and doctors possible. We are trying to create a medical culture shift that recognizes the need for trained nurses in critical care.
What is “sustainable?”
A couple of years ago, I met a USA doctor from a famous USA medical center who told me what I was doing was “not sustainable.” In the meantime, that same doctor trained about a dozen people in her sub-specialty. It will be ten years before the training she did will come into general knowledge. That was a drop in the bucket considering that Nepal has thirty million people. By comparison, CCNEPal has trained 2,300 as of this year, and many of them used their new skills on April 25th, 2015. The nurses and doctors who need this knowledge are the young ones at the beginning of their careers, now working directly with patients. Persons who come to Nepal to train need to find a way to reach a broad audience, and not limit it to the senior doctors doing mainly administrative work. “Train the trainer” is more difficult to do and implement that some might think. I ten words or less: what I do is more “sustainable” than what that other person was doing.
If you are a foreign medical personnel thinking of coming here to train, you are invite to browse this blog.
In past years, I don’t worry too much about what the schedule will be when I get to Nepal. As long as the first few days are scheduled, I know I will get many eager requests to go here or there. The only small city on the 2016 list is Jumla.
Half the population of Nepal lives in Terai. All the medical schools in Terai are non-governmental, i.e., “private” – and I should add, in this region of Nepal there is a higher per centage of Hindi speakers.
Generally, the eleven weeks this time will be divided into two week blocks. As of today, the first eight weeks are spoken for, and I’ll confirm weeks nine & ten soon. The work week in Nepal is six days. I take Saturday off each week. Less travel time = more teaching time.
I plan to post a photo album for each session, on the CCNEPal FaceBook page.
Pokhara ( 1 & 2)
2-day session for MBBS docs and interns May 19th -20th
3-day class for nurses May 22nd, 23rd and 24th; then
another 3-day class for nurses on May 25th, 26th and 27th;
then 2-day course for MBBS, May 29th and 30th;
then 2-day class for MBBS, May 31st and June 1st;
About the town: Pokhara is neck and neck with Biratnagar for the title of Nepal’s second-largest city, with about 353,000 people. It is the jumping off point for many treks, and is situated on one of Nepal’s few lakes. I have taught there twice before, for a total of a hundred nurses. There are two medical colleges in Pokhara. The host is Paschimanchal Community Hospital, Buspark, Prithvichowk, Pokhara. The contact persons are: Dr Umid Shrestha, and Sushila Neupane who now is at Charak Memorial Hospital. (please note that is a correction- I originally gave the incorrect hospital). I will be staying in the city, above and away from “lakeside” while there.
On June 2nd, CCNEPal will travel to the next location.
Bharatpur (3 & 4) – College of Medical Sciences (CMS)
teaching a 3-day class to nurses and/or nursing students on
Sunday-Monday-Tues June 5th,6th and 7th.
then a 2-day session for MBBS June 9th and 10th;
Then another 3-day class for nurses June 12th, 13th and 14th;
and finally a 2-day session for MBBS/interns June 16th and 17th.
About Bharatpur. This city is located where the road from Kathmandu intersects the east-west highway across the Terai. I first taught here in 2011. The city has two medical colleges, the old (“Purano,” also known as CMS) and the new (“Naiyyan,” also known as CMC). I did not know their official names for quite some time. CMS has several distinctions. First, they have the single busiest Emergency Room in Nepal, with a breathtaking level of activity. Next, they serve a population that comes down from Makwanpur, the nearby hill district. Bharatpur is the city closest to Chitwan National Park. Contact person there is Mrs. Sita Parajuli, Matron of CMS Teaching Hospital. Also, Dr Biswas Gurung will know where to find me.
Janakpur ( weeks 5 & 6)
2-day version of class for MBBS, June 19th and 20th (30 seats)
2-day version for MBBS June 21st and 22nd (30 seats)
2-day version for MBBS 23rd and 24th (30 seats)
3-day version for nurses, 26th, 27th and 28th (30 seats)
3-day version 29th, 30th and July 1st (30 seats)
I will leave Janakpur the morning of July 2nd.
About Janakpur. I have not taught here before, but they too have a medical college. Janakpur is the site of the Janaki Mandir, a legendary pilgrimage site for Hindus dedicated to the Goddess Sita. Janakpur is also the site where they filmed this documentary about trains. The primary local language here is Maithili, not Nepali or Hindi.
Biratnagar ( weeks 7 & 8)
2-day version for MBBS July 3rd and 4th (30 seats)
2-day version for MBBS July 5th and 6th (30 seats)
2-day version for MBBS July 7th and 8th (30 seats)
then 3-day version for nurses July 10,11th and 12th (30 seats)
then 3-day version for nurses July 13th, 14th and 15th (30 seats).
I was in Biratnagar summer 2014. That time of year, women apply mehendi. These are nurses who took my class. I worked with “CNEplanet” and enjoyed my time there, despite an auto accident on the way. I returned in 2015.
About Biratnagar. I taught here in 2014 and 2015. It is in the eastern Terai, the largest “industrial city” of Nepal. There is a sizeable Muslim population – the Muezzins start up at about 0430 every day. In 2014 they were having a hepatitis E epidemic, and The New York Times featured Biratnagar in this news video. I believe that this is the city where Lonely Planet wrote: “…there is no reason for any western tourist to ever visit this place.”
So – despite the above statement, I can truly attest to how nice the people are in Biratnagar. They were really super. The host agency is Nobel Medical College with Dr. Bandana Paudel.
I don’t drink the water when I am there. My contact person is Mrs. Dipty Subba.
This is not Dipty’s usual head gear.
Jumla (weeks 9 & 10)
specific dates TBA.
About Jumla. I have a long story about Jumla, but then again, I have long stories about each of these places. Jumla is home to Karnali Academy of Health Sciences (KAHS), in far-western Nepal. I will go there for two weeks, and most likely using the shuttle as opposed to flying. How exactly to rendezvous with the KAHS shuttle, will be one of the loose ends of the summer. It’s on the opposite end of the country from Biratnagar. Biratnagar is twelve hours from Kathmandu by bus, and Jumla is two days by bus or shuttle.
KAHS is new, and the teaching hospital there has 30 beds. They had a fire in one building this past winter, after which patients were treated on pallets on the ground in open air for a few days. They wanted me to go there last year to upgrade skills of emergency and especially pre- and post-op nurses, but this was cancelled after the earthquake. Contact person is Dr. Mangal Rawal. I met him when he was completing his orthopedic residency at Bir Hospital in Kathmandu.
from the KAHS FaceBook Page. The teaching hospital is small and so is the nursing staff.
Jumla has had low rain and crop failure so far in 2016. There are predictions of famine in the district.
After Jumla I will go to Kathmandu. I’ve been asked to do some teaching for an NGO that specializes in “health camps” in the mountains, and other groups. I think by that time, I will need to simply “chill” and enjoy the city.
The above plan is subject to change. It will minimize the bus travel. My 2015 bus accident took three weeks to recover from. Since then I want to avoid the out-and-back trips, designing a circuit instead.
I travel light. Here is my collection of “props” for the class.
I will bring my own supply of “organic coffee.” The locals drink tea here as a rule.
The person who met me at the airport in May 2007 is Mr. Ram Maharjun, manager of Shalom Guest House. He will always know where I happen to be. I will also register with the US Embassy, as in the past.
The best way to follow me is to “like” the CCNEPal FaceBook page.
UPDATED with more specific info Wednesday May 4th and 12th
ACLS training registration can be done at: Registration desk Paschimanchal Community Hospital Buspark, Prithvichowk, Pokhara – 9, Kaski, Nepal. Phone no. 061 530722 Email: pchospital2071@gmail.com
Please share widely.
CNEPal will return to Nepal for ten weeks in summer 2016. We will be in a variety of cities, mostly outside the Kathmandu Valley. Our goal is to create a widespread knowledge of principles of resuscitation and emergency response, throughout Nepal. In the past we delivered 70 sessions of this course, training 2,170 nurses and doctors. Click here for a report: http://wp.me/p1pDBL-yy
We will begin the summer by offering five training sessions in Pokhara Nepal, starting in May.
This course covers emergency response and is modeled after the USA “Advanced Cardiac Life Support” course. (It has been adapted to meet the needs of Nepali learners, and is not the official American course).
In 2013, we did two sessions in Pokhara and trained 95 nurses. There were participants from many hospitals and schools of nursing throughout Pokhara. We hope to have a similar cross section of nurses. Please note: if you took the course before, you are invited to help lead the small groups this time around.
You must attend all days of the session to get the certificate.
UPDATE: Fooding will be included.
Certificate?
Yes, there will be a certificate. It will be beautiful.
This is what the certificate looked like in 2013:
There is a final exam and if you don’t pass the final, you get no certificate.
Hold the date!
2-day session for MBBS docs and interns May 19th -20th
3-day class for nurses May 22nd, 23rd and 24th; then
another 3-day class for nurses on May 25th, 26th and 27th;
then 2-day course for MBBS, May 29th and 30th;
then 2-day class for MBBS, May 31st and June 1st;
On June 2nd, CCNEPal will travel to the next location. We will announce further locations and sessions as they are confirmed.
CCNEPal is an ongoing educational project since 2011. We have trained 2,170 nurses and doctors in Nepal to use a particular set of critical care skills.
May 1st Update
I bought my ticket and I arrive May 16th to TIA. I expect to scurry around Kathmandu doing errands for a day or two then get on a bus outside the Valley. First stop I am hoping for is Pokhara for two weeks.
The Big Audacious Goal
MBBS interns at CMC in Bharatpur. These young docs were willing and enthusiastic. A bright spot for Nepal’s future. In the recent exams, the aggregate scores for CMC were among the highest in the country.
CCNEPal’s goal is to promote cardiac critical care training throughout the entire country of Nepal so that it is “owned” by every medical school and a broad movement of nurses and doctors are comfortable with using and sharing these skills.
Please refer to the report of 2014-2015 activity of CCNEPal to learn my assessment of present capability. The conclusion? Kathmandu Valley has got some good things going, and the best return for the effort will be from work in the Terai.
Half the population of Nepal lives in Terai. All the medical schools in Terai are non-governmental, i.e., “private” – and I should add, in this region of Nepal there is a higher per centage of Hindi speakers.
For those Nepalis thinking about taking the training? It’s easy to find a person who took it before….. ask them if it was worthwhile.
And if you are one of those persons who did take it before… tell your friends. Ask your employer to host the training. I don’t charge a fee, but when it’s outside KTM I do ask for fooding and lodging.
Also – If you took it before – please join me as one of my “assistants” – it’s more fun the second time around.
In May of 2013, CCNEPal started routinely including an anatomy lab in the 3-day session for nurses, to make up for gaps in science preparation ( something I had done in USA for years). For this we obtain en bloc heart-lug assemblies of mutton from local fresh shops. Here’s a shot of the coronary arteries.
Train-the Trainer takes more than just two weeks
We are trying to develop Nepali nurses and doctors to teach these skills and use them in daily practice throughout Nepal, so that it will be “owned” by a wide cross-section of Nepalis. What we do goes beyond the usual “train the trainer” program. The leaders of this course need to be persons who are using the skills in daily practice, but also able to effectively debrief according to what just happened. When we model these skills in class, the participants begin to use them to critique their skills in the clinical setting.
Read past blog entries to get the course objectives, outlines, etc.
CCNEPal uses role play to teach nurses and doctors about situational awareness. These are the actors from the first session at Crimson Hospital in BTWL, May 2015
I will be returning to Nepal for summer 2016. I have not bought my ticket yet, but it will be roughly May 20th to August 10th. As in the past, I don’t schedule sessions of my courses until I get there. I am humbled at the positive word-of-mouth references people give to the training.
General plan
Jumla
I will spend a few weeks at Karnali Academy of Health Sciences in Jumla. This is to fulfill a promise I made to a person who is now passed; but – also a separate promise I made prior to the earthquake in 2015.
I will go to BPKIHS in Dharan; and LMC in Palpa. I wanna go to Janakpur. I will return to Pokhara as well.
Traveling to widely dispersed cities becomes “my other life.” I have friends in all these cities – in some cases they know each other but mostly not – and, people in Kathmandu don’t necessarily know my friends elsewhere…… something amazing always happens on these road trips…. I just don’t know what it will be.
I know it will be hot.
Unlike all the previous places, I know nobody in Janakpur. Anybody out there able to introduce me to Janakpur?
Pokhara? why not! I was there twice before and trained about a hundred nurses.
And yes, somewhere on the way I will teach in Kathmandu.
How to schedule?
So if there are nursing schools, medical schools, or hospitals that wish to host me, please contact me and we will set up some dates. I am especially eager to go outside Kathmandu Valley and to areas I have not been before. send email to: joeniemczura@gmail.com
Maybe this is finally the year I will take a trek……
PS – For those persons in USA – If you are an ACLS-I or PALS-I and you want to help out in Nepal, please contact me. What I do is not part of the American Heart Association, but I know the folks who run the one-and-only AHA ITC in Kathmandu, and they would love to have you affiliate with them.
Final Poster Number on Poster Board: 2.037_HRW Abstract Title: Use of Simulation to Support Role Development for Nurses and MBBS Doctors in Nepal Presentation Date: Sunday, April 10, 16 Presentation Time: 12.45pm – 2.15pm Category/Session name: Poster Presentations: Human Resources and Workforce II Room: Golden Gate Ballroom (Lobby Level)
We hope to see you there.
Impressions
I am blown away by the breadth and quality of the speakers, the tracks,the breakouts, the location, and of course, the other poster presentations. There are at least a dozen other posters about ongoing projects in Nepal.
Paranda
CCNEPal will be giving away trinkets, starting on day one. The specific trinket is a “Paranda” – a hair tassel. (best for people with long hair.)
A paranda looks like this:
It’s braided into a person’s hair. In Nepal it’s very traditional, but these days not worn as often as before. A paranda is “fun.”
Here is a YouTube video showing what this is like. Fast Forward to about 4:24 to see the trick of braiding it on.
I will be giving these away to anybody that talks to me about Nepal. You will be able to find me because I will be wearing a topi, a traditional Nepali cap.
My main goal is to network with people. I don’t take myself too seriously!!
And of course, to read about the CCNEPal project, browse the other blog entries on this site.
Doctor Govinda KC is an orthopedic surgeon from Kathmandu who has been a champion of reform for medical education in Nepal. He is a professor at TU IOM.
Dr KC has made treks to bring medical services to remote areas of Nepal.
He has been willing to dramatize this issue by going on hunger strikes, five times in the past. He’s been able to mobilize medical students at TU IOM. His effort have led to investigational journalism to expose the “medical mafia” of Kathmandu, and also led to the government-appointed Mathema Commission” which produced the “Mathema Report” named after the Chairperson. The journalists have pointed to the involvement of political figures in “buying” the license to run these colleges.
From a previous effort in support of hunger strike of Dr KC. – As of Sept 15th, with all that has happened, it seems so “tame.”
Dr GKC’s most recent hunger strike was September 2015, and he suspended it when the government agreed to an eleven-point list of demands.
Here, as reported in the Kathmandu Post, are the eleven points:
The agreement 1) Form Health Profession Education Commission in the next Cabinet meeting. This Commission will
(a) Formulate Health Profession Policy; (b) Will not renew LoI of Medical Nursing and Dental colleges inside Kathmandu Valley;
(c) Gradually decrease the MBBS seats to 135 then 115 and 100 in next three years; (d) Set Rs 3.5 million fee ceiling for MBBS course; (e) Foreigners should also sit for common entrance examination. For Nepali students they should mandatorily sit for the common entrance before obtaining No Objection Letter and Eligibility Certificate from Ministry of Education and Nepal Medical Council
2) Form a legal commission to probe abuse of authority in KU and TU
3) Form a ‘search’ committee without political representation to appoint office bearers in universities and other health councils.
4) Make the Post-Graduate education free and implement it from this session
5) Take action against owners of Janaki Medical College and properly manage students
6) Government medical college should have 50 percent free seats that should be eventually increased up to 75 percent
7) The government should probe into the extended programme of Dev Daha and Birat Medical College and take action against KU officials.
8) Halt the process of establishing Medical University
9) The ratio of government to private medical colleges should be at least at 1:3
10) Dispatch a letter to KU stating the representation of professors in KU senate.
11) All the above mentioned agreements will remain accordingly, while the rest will be implemented from the action plan endorsed by the Cabinet from: http://kathmandupost.ekantipur.com/news/2015-09-05/drkc-signs-an-11-point-agreement-with-the-government.html
Response by Private Medical Colleges
In September 2015, there was a surprising twist. Within a day, “The Association of Private Medical and Dental Colleges of Nepal” held a press conference, and presented a five-point plan of their own, saying that many medical colleges in Nepal would go bankrupt if the eleven-point plan was implemented. This has been hinted at in the past, but now has been stated more forcefully.
Half the population of Nepal lives in Terai. All the medical schools in Terai are non-governmental, i.e., “private” – and I should add, in this region of Nepal there is a higher per centage of Hindi speakers.
The only list of the five points is in Nepali. Here is a summary from Aug 8th:
Aug 9, 2015-An organisation of private medical colleges has expressed concerns over some of the points in Mathema-committee report, arguing that it would weaken the existing medical colleges and might be detrimental if it is implemented in haste.
The Association of Private Medical and Dental College of Nepal on Saturday asked the government to review the Health Profession Education Policy in such a manner that the ‘fate of private medical colleges are also secured’.
In a statement, association President Dr Bhola Rijal, a senior gynaecologist, has objected to the panel’s recommendations to limit the number of medical seats to 100; MBBS course fee to Rs3.5million; entrance examination for foreign students and to set minimum requirement of 60 percent in common entrance examination to secure an admission……
– The Association of Private Medical and Dental College of Nepal demands a policy review to secure ‘fate of private medical colleges’
– Objects the panel’s recommendations to limit the number of medical seats to 100; MBBS course fee to Rs3.5million; entrance examination for foreign students and to set minimum requirement of 60 percent in common entrance examination to secure an admission
For me, this caused a re-evaluation. Problems in Kathmandu are one thing. There is a distinctly different set of problems faced by medical schools in the Terai.
From Nepali Times. There twenty one medical colleges in Nepal, one third are in the Kathmandu Valley. This map does not include Karnali Academy of Health Sciences in Jumla.
How can the proposals be decided so as to promote medical education around the entire country? The petrol crisis has highlighted the needs of Terai.
Suspended
All of this was put on hold during the Petrol Crisis. But in January 2016 a bill was put up for discussion in the new Parliament that would authorize “Man Mohan Medical College” in Kathmandu to begin construction of a teaching hospital in Kathmandu. This was exactly against the prior agreement with Dr GKC and his supporters and the Mathema Commission.
This is the first of a three-part series of diaries. The next part will review the current status medical education, and the third part will address some other concerns specific to the Terai.
I usually share information about the process of getting a nurse’s license in USA, and I don’t pretend to know about the UK system. The other day somebody shared a link with me that brings you to a paper written by a Nepali nurse in UK who has done research on this subject. Her name is Radha Adhikari. She has done some other writing about nursing in Nepal as well.
it’s titled “The “dream-trap”: Brokering, “study abroad” and nurse.It’s excellent. It’s a bit long, and the best parts are near the end, but if you are serious about the UK, it’s very worthwhile. It goes into the history of nursing in Nepal, and especially the history of nurses who go abroad. Then it covers the whole idea of working with consultancies. And it is very honest about the problems that nurses face once they get to UK.
Ms. Adhikari did her PhD work on this subject. Here is the abstract for her doctoral dissertation:
The migration of nurses is stimulating international debate around globalisation, ethics, and the effects on health systems. This thesis examines this phenomenon through nurses trained in Nepal who migrate to the UK. Since 2000, increasing numbers of Nepali nurses have started crossing national borders to participate in the global healthcare market, particularly in the affluent west. By using qualitative multisited research and in-depth interviews with key stakeholders in both Nepal and the UK, this thesis explores why nurses aspire to migrate, how they fulfil these aspirations, and their experience of living and working in the UK. The thesis begins by examining the historical development of nurse training in Nepal, particularly from the mid 1950s. This period saw profound socio-political transformations, including in the position of women in Nepali society and in the perception of nursing in Nepal. Previously, many families were very reluctant to send their daughters into nursing. By the late 1990s, middle-class women and their families were increasingly attracted to nursing, both as a vocation and as a means to migrate. The thesis explores the rise of private training colleges to meet the increased demand for nurse training, and the new businesses that have grown up around the profession to facilitate nurse recruitment and migration. Around one thousand nurses have migrated to the UK since 2000, and the second part of the thesis presents their experiences of the migration process and of working and settling in the UK. Nurses have faced complex bureaucratic and professional hurdles, particularly after UK nurse registration and work-permit policies changed in 2006. The thesis also highlights how highly qualified nurses with many years of work experience in Nepal have become increasingly deskilled in UK. Frequently sent to rural nursing-homes by recruiting agencies, they create and join new diasporic support networks. Further, many have left their loved ones behind, and experience homesickness and the pain of family separation. Often, they plan for their husbands and children to join them after several years, and the research explores this and the issues faced by their families, as they relocate and adapt to life in the UK. Finally, the thesis makes some important policy recommendations. For Nepal, these relate to greater regulation of nurse training and the brokering of nurses abroad. In the UK, they relate to increasing the flexibility of registration and visa regulations to assist in supporting Nepali nurses’ work choices, and to value and utilise their professional skills in the UK better. to find the entire PhD work, go to: https://www.era.lib.ed.ac.uk/handle/1842/6199
This has been in print for awhile, obviously but I only just found it. Dr Adhikari’s email is in the profile linked above.
Please help me improve this blog entry. I know it’s not perfect but it’s a news item many Nepali nurses are interested in.
preparing the banner for the march.
Nepali Nursing Students need to read this before enrolling in nursing education in India
If your plan is to study nursing in India, then work in India or go to a third country such as Oz, watch this video. Click here. Or click here for another one. Please share these.
It is especially important to share this with young people thinking of going to India, before they spend any money.
Because I go back and forth from USA to Nepal, nurses ask me about working “abroad.” (to see what I have written, click here). Turns out that many young women study nursing because they hope to get out of Nepal, and go to India, UK, EU, Oz, or – anywhere. I have noticed that since the blockade these are getting more hits. I will write about this in some future blog.
At this time there are said to be 10,000 Nepali women per year graduating from nursing in various Universities in India. Since each program takes at least three years, this adds up to 30,000 people affected. I recently learned about a new problem. See the letter below.
Here is the letter from the India Nursing Council. This issue extends back in time well before the blockade.
I learned that a group of Nepali nurses were meeting with the Nepal Nursing Council, and planning a protest. I queried the person who informed me about it. Here is her reply:
We are deeply concerned with the reports that Nepalese nursing students graduated from Indian Nursing colleges are denied registration by Indian Nursing Council. This is clearly a breach of “1950 India-Nepal Treaty of Peace and Friendship” that grants the Nepalese and Indian citizens to live and work in either of the country. Thus, by denying the registration, Indian Nursing Council has barred Nepalese nursing students from pursing Nursing career in India which is totally against the aspiration of the treaty. Also, without registration from parent council, Nepalese nursing students who have graduated via Indian nursing colleges are unable to apply nursing jobs abroad and thereby are restricted from pursuing career abroad despite of meeting all the other parameters.
A protest by Nepali nursing students in Bangalore, India.
She continued:
India has been a lucrative country for Nepalese students to pursue their study and nursing, top the list. This has not only given an opportunity for Nepalese students to acquire best education but also has opened up business opportunities for many Indian institutes, and the new provision, barring Nepalese nursing students from getting registration will surely jeopardize the business opportunities that nursing colleges from India are enjoying so far, as such discriminatory provision will discourage Nepalese students to prefer India for nursing hereby. Nepal-India relationship has been very special in every aspects and are two very reliable partners from the region, who have strong potentials of working together in making the region a better place. The growing demand of healthcare workers in both countries can only be fulfilled by respecting and acknowledging the value of these healthcare-related students and discovering the ways to assimilate them, which anyway Nepal-India treaty of peace and friendship guarantees. So, this is our humble request to concerned authorities and departments to respect the century-old Nepal-India relationship, diligently adhere with the provision of 1950 India-Nepal treaty that guarantees equal job opportunities for both nationalities, willfully acknowledge the importance of Nepalese nursing students and value their skills and potentials, and weigh this sensitive issue wisely and pragmatically and do the needful.
placards used in the protests.
Finally,
Reportedly, there has never been an issue in this regard in the past and there shall be no issue restoring the earlier provision, that is, registration opportunity for Nepalese nursing students graduated from India. We believe the grievance will be heard and dealt by in earliest possible. #source kagmandu magazine
The nursing students wrote letters to the Nepal Nursing Council and the Nurses Association of Nepal. Click here to read it.
There was an article in a Bangalore newspapers
[अशोक महर्जन]
काठमाडौँ, २३ कात्तिक । ‘भारतमा नर्सिङ विषय नपढौं’ भन्दै भारतमा नर्सिङ विषय अध्ययन पुरा गरेर फर्किएका नेपाली विद्यार्थीहरु सोमबारदेखि आन्दोलनमा उत्रेका छन् । आन्दोलनको क्रममा विद्यार्थीहरुले सोमबार भारतीय दूतावास अगाडि धर्ना दिएका छन् । धर्नास्थल पुग्नुअघि नेपाली विद्यार्थीहरुले भद्रकालीदेखि ¥याली निकालेका थिए । – See more at: http://onlinepatrika.com/62684/#sthash.i3fOAUbu.otIDopgS.dpuf
Will the Nepal Nursing Council help?
I was previously aware that the Nepal Nursing Council was not enthusiastic about granting Nepal nursing registration to newly-graduated Nepali women who wished to work here. One person from NNC told me “Those schools in India are not as good as Nepal nursing schools. Not enough practical.” The NNC has not made it easy. Historically, there are many nurses in Nepal who attended nursing school in India – and who are in fact, Indian citizens. (more of these work in Terai. Nurses from most parts of Nepal speak at least a little bit of Hindi).
Will the educational consultancies in Nepal help?
This is a good question. One person in the discussion said she thought the consultancies on Putalisadak, where many people go for career advice, do not wish for this to become widely known, since it will affect their profits.
Will the Nepal Government help?
The Nepal government presently has other more pressing diplomatic problems to discuss with the India government. Somehow I worry that they are not in a position to advocate for Nepali citizens working or studying there as effectively as in the past. It occurs to me that no Nepali journo has explored what’s happening to Nepali people in India these days.
In November 2014 on my epic India trip, I was invited to teach at a school of nursing in Bangalore. At this place they were not so rigid about identical uniforms. I enjoyed the colorful Punjabi outfits. The students were smart and enthusiastic and reminded me of USA students.
.
Please share widely. I am likely to edit this and improve it with feedback from people who have personal experiences or who are involved in addressing this problem.
Now that I am back in USA, I have been blogging on DailyKOS, a website with a million subscribers, to which I occasionally contribute since 2008. I’ve been blogging there every day since the petrol crisis began a few weeks back. Here is my reaction to the Human Rights Watch report.
At the end of the Human Rights Watch report, is a list of recommendations. Keep reading to the bottom, because I will add some items at the end, that I think were overlooked.
Here are the recommendations from HRW:
IV. Recommendations
To the Government and Security Forces
Ensure that all security forces abide by the UN Basic Principles on the Use of Force and Firearms by Law Enforcement Officials.
Immediately end the indiscriminate and excessive use of force, and ensure the intentional use of lethal force only occurs where strictly necessary to protect life.
Immediately establish an independent commission of inquiry to investigate the unlawful killings of protesters and police.
Ensure that these findings are forwarded to the Attorney General’s office for prosecution.
Ensure that those accused of violence and other crimes during the protests are accorded full due process rights, including a fair trial, freedom from torture, and access to lawyers and family. Ensure that any statements given by the accused under duress are not introduced as evidence in court.
Immediately end the harassment and intimidation of members of the public belonging to the Tharu and Madhesi communities, including beatings, threats, and the use of racial slurs by members of the security forces.
Ensure full protection of political rights, including freedom of assembly, association, and speech.
Undertake a broad consultation with all aggrieved communities and stakeholders to redress rights violations.
Take immediate steps to address any systematic discrimination suffered by minority communities, including providing effective judicial remedies to afford redress and accountability for rights violations.
Issue clear instructions that anyone holding public office at any level who engages in hateful speech or incitement of serious crimes will face significant consequences, including investigations and dismissal from public office, and possible criminal prosecution if found to have incited crimes.
Ensure all security forces comply with the Ministry of Education’s 2011 “Schools as Zones of Peace National Framework and Implementation Guideline.”
To the Protesters and Protest Leaders
Publicly call on all protesters to desist from violence and other crimes.
Fully cooperate with the police and others in any criminal investigation into serious crimes.
To the International Community
Urgently press the Nepali government to abide by its international obligations not to use excessive force in policing demonstrations and to abide by the UN Basic Principles on the Use of Force and Firearms by Law Enforcement Officials.
Press the Nepali government for timely and credible investigations of alleged human rights abuses, and for perpetrators among both the security forces and agitating groups to be prosecuted.
Strengthen the capacity of international human rights monitoring inside Nepal, including by pressing for access by the Office of the High Commissioner for Human Rights (OHCHR).
Be alert to activities or rhetoric which may contribute to human rights abuses, and strenuously dissuade any actor from taking this course.
My critique
I certainly agree with the recommendations above. HRW seems to be clearly supporting the idea that the government needs to negotiate and compromise with the protesters. The other day a rally in Birgunj attracted 100,000 supporters. If the government plans to use riot police again, it will find that it takes a very large number of riot police to dominate a crowd that size. This has grown well beyond what can be controlled by force.
The ICRC publication I think people in Nepal need to study is:
Ensuring the preparedness and security of health-care facilities in armed conflict and other emergencies
Date of release: Jul 27, 2015 Languages: English
This publication is intended as a practical manual for governments, hospital managers and others concerned, with a view to helping them prepare for and manage situations that could jeopardize their objective of assisting the wounded and sick and maintaining the health of people affected by armed conflict and other emergencies. Built on the recommendations that emerged from two Health Care in Danger experts’ workshops on ensuring the safety of health-care facilities, which took place in Ottawa, Canada, in 2013 and Pretoria, South Africa, in 2014; this publication has also benefited from contributions by the Canadian Red Cross Society, the Egyptian Red Crescent Society, the Harvard Humanitarian Initiative, the International Federation of Hospital Engineering, the International Hospital Federation, Médecins Sans Fontières, the Pan American Health Organization and the World Health Organization.
Chapter 1 gives an overview of the impact that violence may have on the delivery of health care, highlights the importance of enhancing the security of health-care facilities and discusses the protection afforded by international law.
Chapter 2 focuses on contingency planning for health-care facilities, measures to enhance coordination and cooperation between facilities, and advocacy for the safe delivery of health care.
yy Chapter 3 covers issues relating to the security and well-being of health-care personnel and patients, and methods for preparing for and dealing with stressful situations caused by an emergency.
yy Chapter 4 discusses a number of generally recognized architectural principles and engineering considerations relating to the design of health-care facilities and proposes measures that could increase the security level of infrastructure.
yy Chapter 5 outlines potential risks of disruption in the supply of health-care equipment and goods, and proposes measures to enhance the preparedness and resilience of health-care services.
yy Chapter 6 considers the implications of temporarily relocating health-care services to a safer place when security for staff and patients reaches a higher risk level
My additional items:
For the riot police:
1) arrange for the presence of an ambulance at or near the scene of riot control actions so as to minimize the transit time to medical care for any injured persons.
2) issue first aid kits to each unit in a riot control action and train members of each squad in their use especially to control hemorrhage.
1) improve security by obtaining the recommendations from iCRC in their “health care in danger” initiative and implementing them.
2) train staff in situational awareness, mass casualty triage and tear gas decontamination.
For protest groups
1) use smartphone video cameras to document all encounters.
2) train as many protesters as possible in first aid techniques, especially control of hemorrhage.
For all sides
1) respect the neutrality of hospitals, medical personnel, ambulances and first aid providers.
2) medical schools and hospitals in the Terai and elsewhere need to ramp up courses of elementary first aid to police and to potential protesters or protest groups.
I would note that on YouTube, there are videos of many of the incidents described in the report, as well as others dating back months or years prior to the current round of protests. It’s clear to me that some of the wounded in the videos died of hemorrhage, and it is equally clear that the fellow protesters and police had no idea whatsoever, how to use elementary first aid techniques to control bleeding. Some of the deaths were easily preventable after the initial wound. Of course, all of the death were preventable if they protests had not taken place; but if protests are planned, some attention to treatment of casualties needs to be considered.
I will add to this in coming days. If the readers wish to add something, feel free.
I have more than one blog, and this is the one that describes, in professional terms, “CCNEPal” the critical care education project in Nepal that I started in 2011. Please feel free to browse the site.
Nurses need to learn how to do this. (don’t try this at home. these are trained professionals under expert supervision)
There’s a list of blog entries to the right, as well as helpful links to nursing in Nepal. In Nepal I explain USA to the Nepali people I work with. In USA, I explain Nepal to Americans.
Yes, I was in Nepal for the earthquake.
Sangkhu Nepal. Yes, I was in Nepal for the April earthquake but I travel a lot and I was nowhere near the epicenter.
I knew that Kati Kleber, RN, the author of “Becoming Nursey” was going to print a review of my book, and I was pleased to read it today. She was so enthusiastic she made me want to read the thing myself ( and, I already know how it ends!)
Required reading for every medical person who thinks he understands what goes on in Nepal…… available on Amazon at http://www.amazon.com/dp/1632100029
I realize that the most recent entry prior to this one was on the care of patients with injury due to “Rubber Bullets” used in riot control actions by police in Nepal. They are having political turmoil, a sad echo of the drama described in my book, The Sacrament of the Goddess. I needed a better entrée page – here it is!
Also, I thought her advice for new RNs in Becoming Nursey was right on. It’s been great to follow her blog, and you should do so if you haven’t already.
Brad Wong photo, 2008. women’s inpatient ward. eleven women, one bathroom.
June 4th 2020 Update after George Floyd protests in USA – I wrote this five years ago and the medical details are unchanged. Needless to say, #BlackLivesMatter and now the right to peaceably assemble is being challenged in my own country. I added one noteworthy medical picture to this but the rest still applies. From a purely technical viewpoint of handling firearms, it is crystal clear that police agencies across USA are not trained in this weapon and are not using it properly. I have been considering writing more about riot police tactics, maybe in coming days I will. These protests are not going away.
note: be sure to click on the colored words. they are hyperlinks.
News from Bhairawaha
In USA we have ample access to firearms, and there are many nurses and doctors (including me) with experience with ballistic wounds of all kinds. Starting in 1977 when I worked at Boston City Hospital (where the police took every gunshot wound victim), I have dealt with this. In Nepal, not so much. Nobody here owns a firearm. (which is a very good thing!)
Tutorial needed
As the violence continues in Terai, I am thinking that every nurse and doctor needs a tutorial on treatment of wounds from bullets – both the “usual kind” made of lead and steel, and the “Rubber Bullet.”
Rubber bullets (also called rubber baton rounds) are rubber or rubber-coated projectiles that can be fired from either standard firearms or dedicated riot guns. They are intended to be a non-lethal alternative to metal projectiles. Like other similar projectiles made from plastic, wax, and wood, rubber bullets may be used for short range practice and animal control, but are most commonly associated with use in riot control and to disperse protests.[1][2][3] These types of projectiles are sometimes called baton rounds.[4] Rubber projectiles have largely been replaced by other materials as rubber tends to bounce uncontrollably.[5]
Such “kinetic impact munitions” are meant to cause pain but not serious injury. They are expected to produce contusions, abrasions, and hematomas.[6] However, they may cause bone fractures, injuries to internal organs, or death. In a study of injuries in 90 patients injured by rubber bullets, one died, 17 suffered permanent disabilities or deformities and 41 required hospital treatment after being fired upon with rubber bullets https://en.wikipedia.org/wiki/Rubber_bullet
There are different styles of “rubber bullet”
A properly trained policeman is supposed to fire the rubber bullet at the ground in front of the protester, so it only hits the protester in the legs.
If it hits you in the eye, you will lose your eye.
If it hits a child, it can kill – we already knew this. Everybody already knew this.
If you see a policeman with a gun that has a wide mouth like one of these, it means they are ready to use rubber bullets:
pix paul lewis/http://www.dailymail.co.uk/debate/article-2059053/The-decision-authorise-use-plastic-bullets-bad-wrong.html I don’t know for sure this is the style that is being employed in Nepal.
When you see the shooter raise it up, protect your eyes. They don’t spend a lot of time aiming it, they are more accurate than you think, and the projectile travels faster than you expect. Protect your eyes!
If the riot police team was well trained they limit who gets to use this. I notice that these are being issued indiscriminately and used willy-nilly. Even if you accept the premise that non-lethal rounds have a place, this is still not okay.
This is from the Kashmir study. If the wound looks like this, it’s an ENTRY WOUND and the projectile is inside the body.
I looked for a specific video on medical treatment of wounds from rubber bullets. Here is a video of what it is like to get hit with one: https://youtu.be/djtnh5vonz8
Doctors and Nurses in Terai need to watch this next video and learn more about projectile injuries
I did find a six-minute video on assessment and treatment of bullet wounds. In USA we have ample access to firearms, and so many people (including me) have experience with these. In Nepal, not so much. The size of the external wound has no relation to the amount of internal bleeding the victim is having.
I would be remiss if I only focused on the medical treatment and made no other comment.
Flashbangs – June 9th UPDATE
There are other “nonlethal” devices used by police. Here is an article on “flashbangs” from a magazine for police.
Lessons
The protesters should not be bringing children to these events, or allowing them outside. Would you allow your child outside if a tiger was in the neighborhood?
The police need proper training in use of these weapons.
Escalating violence by throwing stones, invites a police response. The police and the Army, can be counted on to escalate until they dominate. It is foolish to expect them to do otherwise. They only way they will go away is when people stop provoking them. Express your anger in a different way, such as by voting.
When you see the police like this, go away from there. It’s simple, really.
Everyone needs to be able to identify “escalation” and “de-escalation” and learn how to de-escalate.
This whole cycle got out of control when the people in Tikapur made a conscious, cold-blooded decision to murder Nepali police that were trying to keep things peaceful. Violence only begets more violence.
“This is not just the issue of Dang, people in other parts of country presently fear loss of existing social and communal harmony,” Shanta said. “There is a dire need to voice for restoring and maintaining communal and social harmony in all parts of the nation.”Baharu Tharu, another participant in the rally, expressed worries on the probability of conflict between the Tharus community members and the hill people community. “People from all caste, religion, ethnicity and region should live in harmony. We have helped each other in hard times and must continue doing so in future also,” he said. “As social beings it’s not possible to live in society without helping each other.” – See more at: http://myrepublica.com/society/story/28150/tharu-organize-rally-in-dang-for-social-harmony.html#sthash.TYUG5dX0.dpuf
from Republica. Dang, in western Nepal. These are the women of the town. It seems like the young boys are the violent ones. let’s pray for all the cooler heads to prevail. The world will not end Spet 21st just because the new constitution will be announced Sept 20th
The new constitution will be announced Sept 20th, and nothing will change that. On Sept 21st, everyone will arise in the morning and look out the window. The world will still be there and it will look the same.
Finally, the factors that go into “communal violence” (e.g., “a riot”) are complicated. In Nepal, I work in this issue because it is prevalent – long before the widespread protests in Terai region. My second book addresses the question as to why and how this happens, and how nurses and doctors get mixed up in it.
Right now I am not exactly with Dr KC even though I agree with him that things need to be fixed and brought out into the open. Dr KC is a positive and inspiring role model. The members of the Mathema Commission also included some other top guys who also have fought against corruption in the medical sector.
The Mathema Report
The effort to reform medical education financing in Nepal needs to focus on more than just the Kathmandu Valley.
What this blog is not about
I’m not going to recapitulate the entire history of Dr. Govinda KC’s hunger strikes, or the buying and selling of licenses to operate medical colleges, or the allegations of corruption at the highest level, or bribery required to obtain a seat at one of the more prestigious Medical College post-graduate programs, or the Medical Mafia, or the likelihood of implementation of the Mathema Report.
If you are a bideshi reading this, it seems – messy. That’s because it is.
The problem?
It’s best illustrated with the following diagrams, originally from The Nepali Times in April 2015.
There twenty one medical colleges in Nepal, one third are in the Kathmandu Valley.
The above diagram omits the Karnali Academy of Health Sciences, in Jumla (mid-western, not in Terai. It’s new.)
Here is another, more striking diagram:
Half the population of Nepal lives in Terai. All the medical schools in Terai are non-governmental, i.e., “private” – and I should add, in this region of Nepal there is a higher per centage of Hindi speakers.
One of the key objections of the #IamWithDrKC movement has been the announcement that two (or three? or four?) more medical colleges would be granted permission to open in Kathmandu. High level politicians have invested in these and money has changed hands.
Another way to look at the number of colleges in Kathmandu by comparing with Delhi. I agree with those who say there are already too many
Dr KC had an eleven-point agreement with the government, just last week ( Sept 8th). The next day, the Association of Private Medical and Dental Colleges of Nepal held a press conference to register their objection. At present, the government has pledged to bring all parties back to decide the next step. (this is exactly what the government would do if this was the USA).
Now, I don’t pretend I know all the details, but I do know I have traveled outside Kathmandu Valley and I have taught doctors and nurses in Terai and the hills. Of the 2,130 people I trained, more than half were from outside Kathmandu. Half of Nepal’s population lives in Terai.
-The teaching hospitals of these schools in Terai are critical to the health of people in Terai. Every one of these is doing rural outreach and medical camps to the surrounding region as well as the hills such as Makwanpur. Before these schools were established, people of the terai needed to go to Kathmandu for sophisticated treatment. (they still do need to go to Kathmandu in some cases, but not as much).
– The supply of MBBS doctors who will do service in rural areas for debt forgiveness is greater, due to these colleges.
– colleges such as Chitwan Medical College are producing graduates just as skilled as those coming from TU or KU.
This summer Nepal had widespread protests in Terai about unfair treatment, and for those who have been to Terai the contrast between Terai and Kathmandu is dramatic. Many more living in poverty in Terai. It’s only in the past dozen years that medical care has become more widely available there. If Nepal closes the private schools in Terai , the availability of care will be taken away. Reports in the newspapers indicate that the government-run medical schools are just as corrupt, so converting the privately run schools will not improve things. Look at Bir Hospital: they are run by the government, and the problems caused by lack of funding there are quite well known. Same with the zonal hospitals.
A complete government takeover will result in eleven more places that are dramatically underfunded, like the zonal hospitals. Is that what is wanted?
For these and other reasons, I think that any plan should be careful not to destabilize the medical education outside the Kathmandu Valley. (I’m not saying it’s perfect). The summer andolans over the constitution in Terai are not ended. Let’s not give the people of Terai one more reason to be unhappy.
One little thing I would add to the already long list of what I would like to see:
I was at one place outside Kathmandu where they told me: You are the only foreigner who has ever come here. When I’ve been to many of the places in Terai they tell me “You’re not just the only foreigner, you are also the only one who comes here from Kathmandu to teach us.”
On Planet Earth, in “the west,” there is a long tradition of visiting medical professors. Nepal does not quite participate. (the ones who come from India have been criticized, which I think is unfair. It’s easy to bash India, this should not be so freely seized as an opportunity to join in). There is a longstanding practice of having videshi doctors visit Nepal, and yet they all seem to congregate at just a few of the schools in Kathmandu. Or in many cases, they spend time in a village in Solu Khumbu (for example), reliving some fantasy of what Nepal used to be like but has now outgrown. Now, the villages of Solu Khumbu need medical care, but – is this the best way to provide it? Nepal is increasing urban.
It’s all too often that when foreigners come to share knowledge, they do so by only teaching a dozen or two dozen people in Kathmandu. Nepal could benefit from systematizing this somehow, and spreading it around.
I think more effort should be made to develop connections between each school and those foreigners who bring medical expertise.
There’s clearly been a massive expansion of MBBS education, and in a few years these same men and women will all apply for post-graduate courses as an MD. Right now, the medical establishment needs to plan for this, and create slots.
In summary, I want to support Dr KC but I think the schools from the Terai have valid points that need to be included.
Every nurses and doctor in Nepal has probably already heard about the patient that was thrashed and killed by a mob in eastern Terai Friday.
(Kathmandu) The Red Cross in Nepal expresses its deep concern at increased incidents of vandalization of ambulances in relation with ongoing demonstrations in Terai/Madhes in the past four weeks. The incident that happened on 11 September 2015 at Sonukhada of Mahottari district has astounded the Red Cross – an injured person in need of urgent medical care was taken out from the ambulance and killed; the ambulance was then torched. https://www.icrc.org/en/document/nepal-injured-people-and-medical-transports-must-be-protected-all-circumstances
“Astounded” is not a word or phrase that the Red Cross uses lightly.
Yes, the man was a police member. Yes, he was also a dalit – a member of a caste that has suffered poor treatment; YES, he was a family man with two children; and a son. But most of all, he was a Nepali citizen from Nepalganj who was defenseless. He already had twelve stitches on his head.
Cadre
Here is a small thing that has bothered me. The young men and boys who participate in these demonstrations are often called “cadre” in the newspapers. This is not the right word. “cadre” implies that they are politically indoctrinated and trained –
: a nucleus or core group especially of trained personnel able to assume control and to train others;
These guys are far from trained and disciplined. Can we find a better name? Maybe “follower” or something like that. “Cadre” elevates them higher than they really are.
Some questions about the police decisions
Why was there no police escort? Why was the ambulance the only vehicle? How did the mob on the side road know he was coming? Will the police and army now take additional steps to make sure their vehicles are safe?
Click here to read a news account of the way that businesses and factories are being targeted in Biratnagar, the industrial heart of Nepal.
Moreover, the State needs to think about the scale and nature of the escalating protest. The situation is more dangerous than the State thinks. Most of the rural areas of Nawalparasi, Kapilvastu, Rupandehi, Parsa and Bara are extremely tense. Because of the excessive use of force by police, people are angry and more violence can erupt at anytime. So far, 31 people, including 10 police officers, have been killed due to the ongoing protests and resultant violence. And, violence only seems to be increasing in Nepal’s Terai. Click here to find the field report prepared by the Terai Human Rights Defenders (THRD) Alliance about the reality of violence in Terai in the last 2 weeks. http://www.humanrights.asia/news/ahrc-news/AHRC-STM-152-2015
Long before this happened, I was teaching about a skill known as “situational awareness.” After reading the statement from the Red Cross, I decided to Google the Red Cross and see if they had any recommendations about ambulance safety.
About the Red Cross and Ambulances
The Red Cross works in Africa and the middle east, and the situation is different there. Syria, Yemen, Somalia, and places where armies are using machine guns and artillery supplied by outside countries. Suicide bombers are active. These are active war zones, and military weapons are widely available. The bloodshed here in Nepal is shocking to people in Nepal because it goes against the image we all want to have, but on the scale of things Nepal is not as out of control as these other parts of the world, where for example, fifty people per day may get blown up.
For nurses and doctors?
The psychological toll of being threatened by violence, such as when you are working in an ER, is tremendous. In the long run, nobody will want to work in affected areas. People will get out.
Health Care in Danger project
The Google search led me to the section of the ICRC site that deals with ambulances and hospitals that get caught in the middle.
Towards a solution : The Health Care in Danger project
Health Care in Danger is an ICRC-led project of the Red Cross and Red Crescent Movement scheduled to run from 2012 to 2017 and aimed at improving the efficiency and delivery of effective and impartial health care in armed conflict and other emergencies. This will be done by mobilizing experts to develop practical measures that can be implemented in the field by decision-makers, humanitarian organizations and health professionals. https://www.icrc.org/eng/what-we-do/safeguarding-health-care/solution/2013-04-26-hcid-health-care-in-danger-project.htm
Browse this link
On the ICRC site, are links to a dozen or so publications related to this.
The Red Cross has some videos as well. These tend to focus on Africa. The first is short -just 3 minutes and 21 seconds. Health Care In Danger: Seeking solutions videohttps://youtu.be/tknwQDlZx2I
In this thought-provoking event, part of the ICRC-led Health Care in Danger project, the panel discusses a range of practical steps that can be taken to address the critical humanitarian challenge of violence against medical care, and save the lives of thousands of people around the world. Featuring speakers Dr Bruce Eshaya-Chauvin Medical Advisor, Health Care in Danger Project, ICRC Geneva, Paul McPhun Executive Director, Médecins Sans Frontières – Australia, Dr Sarah Miller Clinical and Forensic Psychologist & delegate with the International Red Cross Red Crescent Movement.
The recommendations are similar to things I already described in past blogs. Not every preventative measure applies to Nepal, but it gives examples of how to plan.
Please everyone step back and stop and think of who you are hurting. Like everyone else who is following the news, I want the violence to end. From the beginning I have thought that all parties needed to talk and be open to dialog. I am holding my breath, hoping that things will calm down. Further problems in Terai will impact every doctor and nurse, and certainly make it harder for every one who needs a doctor or nurse.
from http://setopati.net/society/9168/ Whenever anything happens in Nepal, a crowd gathers. The two guys who beat the doctors were arrested. This is progress!
The dispute was about who should pay for an ambulance at time of discharge.
A nurse at the hospital told Setopati that Silwal was asked by the doctors to arrange for ambulance after his ward, who was admitted at the hospital for the treatment of jaundice, was discharged. However, Silwal entered an argument with the doctors saying that it was the duty of hospital and not patient’s relatives to arrange for ambulance. The nurse said that Silwal was on his police uniform, and changed his clothes before beating the doctors. Lalitpur Police has arrested the alleged with the help of the relatives of other patients in the hospital. The brother-in-law of the policeman, who was with the accused, was also held by the police. Meanwhile, the patients admitted at the hospital have been affected after the doctors at the hospital came out to protest the incident and demanded action against Silwal. – See more at: http://setopati.net/society/9168/#sthash.rpZKTCgz.dpuf
The doctors are not to blame. This is all too common at hospitals in Nepal.
Patan Hospital is well-respected and hosts the Patan Academy of Health Sciences, a medical school. Due to it’s previous affiliation with UMN, PAHS still enjoys a higher number of videshi exchange students than most other hospitals in Nepal. Patan Hospital is not immune from angry “patient parties” and neither is any place in the whole country.
Situational Awareness is the key term.
It means, it’s not enough to treat the patient’s illness. You must also address the mental state of the family.
CCNEPal uses role play to teach nurses and doctors about situational awareness. These are the actors from the first session at Crimson Hospital in BTWL, May 2015
ask the Ministry of Health and Populations to add “violence prevention training” to the national health plan.
make sure you know how to contact the police.
if you are an MBBS student, ask your medical college to sponsor CCNEPal’s training so you can be prepared for this scenario.
In USA lately, whenever violence happens, the bystanders now start recording on their cellphone. Why not use this in Nepal?
always publicize the incidents, so we can get an accurate idea of how frequent and widespread this problem is.
CCNEPal is presently dormant while the principal faculty is back in USA. send an email to joeniemczura@gmail.com to request future training.
MBBS interns at CMC in Bharatpur. These young docs were willing and enthusiastic. A bright spot for Nepal’s future. In the recent exams, the aggregate scores for CMC were among the highest in the country.
Note about CCNEPal:
CCNEPal was in Nepal from 2014-2015 to teach critical care skills including “patient party counseling” to nurses and doctors. We have taught this at four medical colleges, as well as other locations. CCNEPal was privately funded for that period of time. The funding ran out and CCNEPal returned to USA. We have a proposal to return and set up a system for all MBBS programs to teach these skills, but we await further funding. CCNEPal has worked with a company in USA that specializes in NGO funding, and they tell us that if a government agency in Nepal were to add this to the health priorities and request an international group to fund it, we could then continue. If you are an MBBS student, please ask your medical college to join this campaign. Ask them to send me an email – joeniemczura@gmail.com Share this message.





 This is a book review of
This is a book review of 






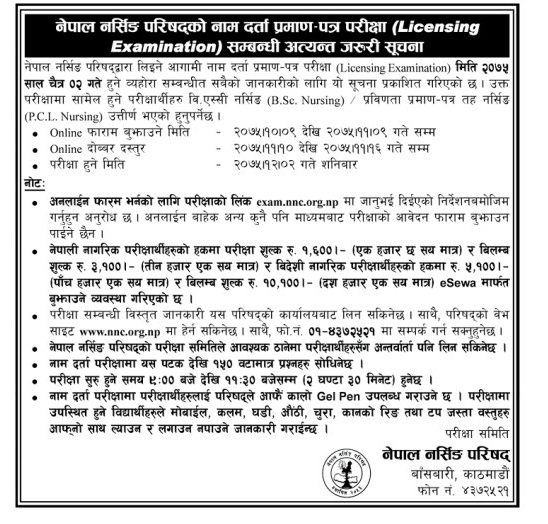












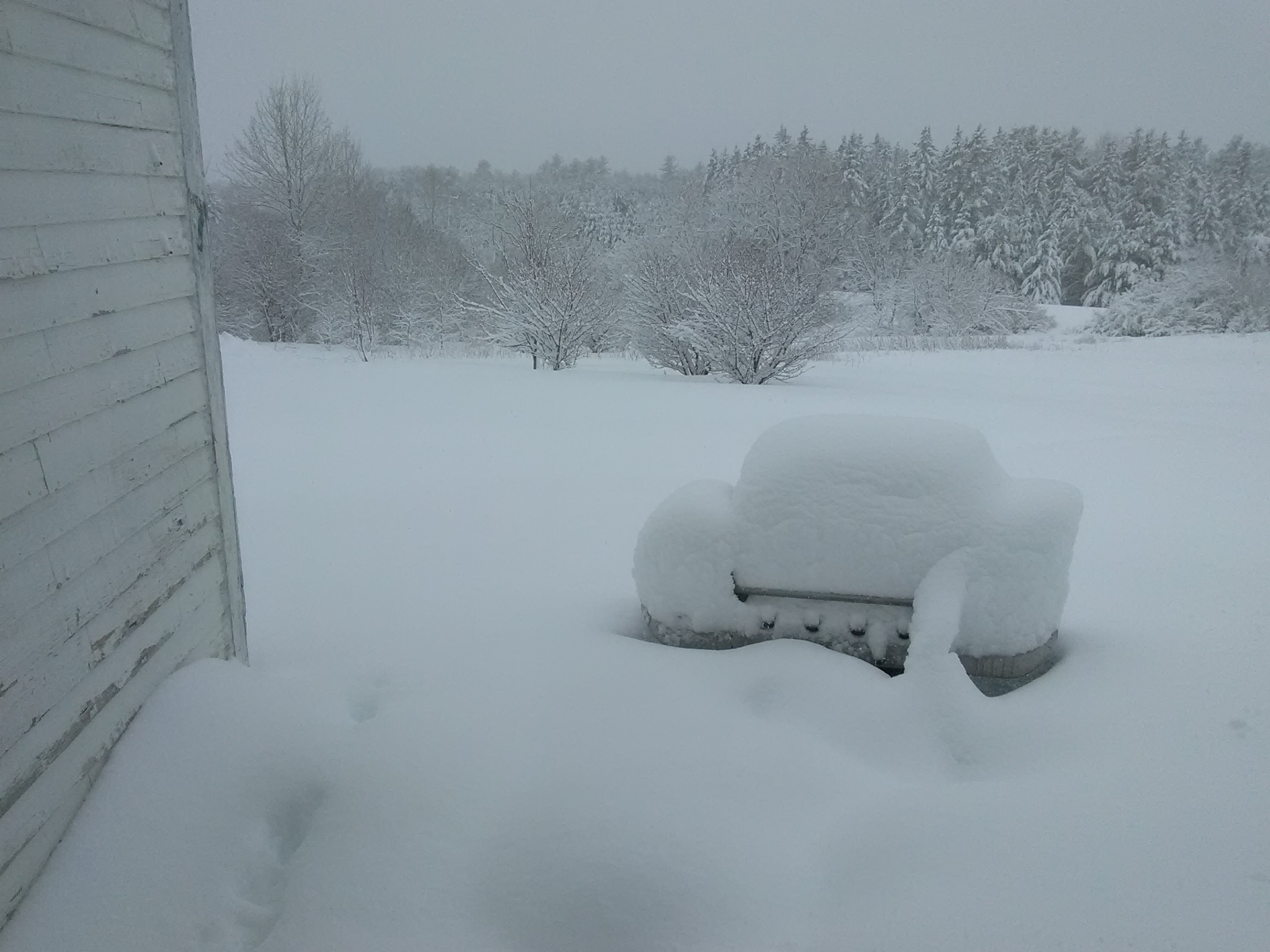
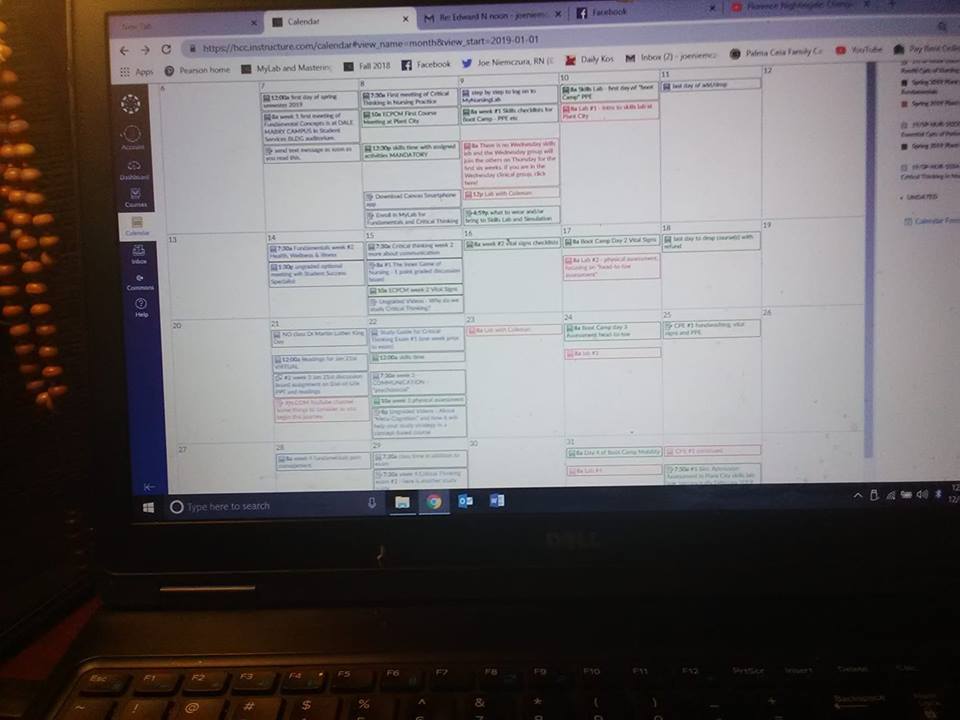




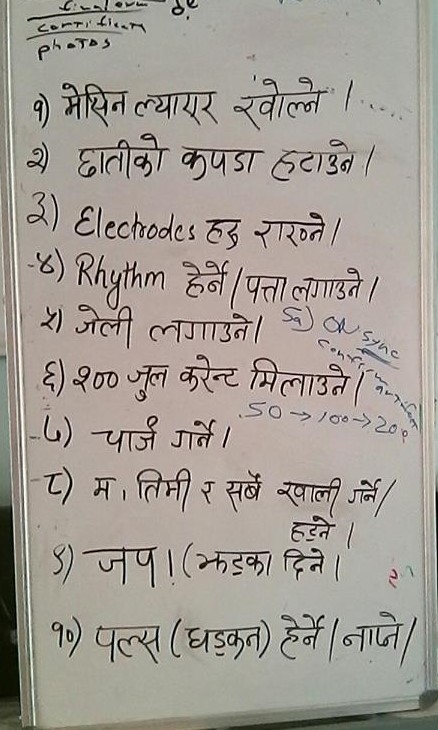



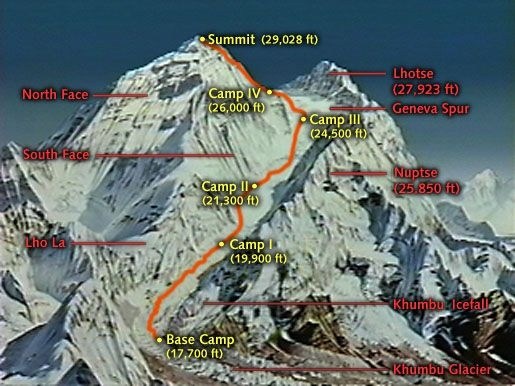









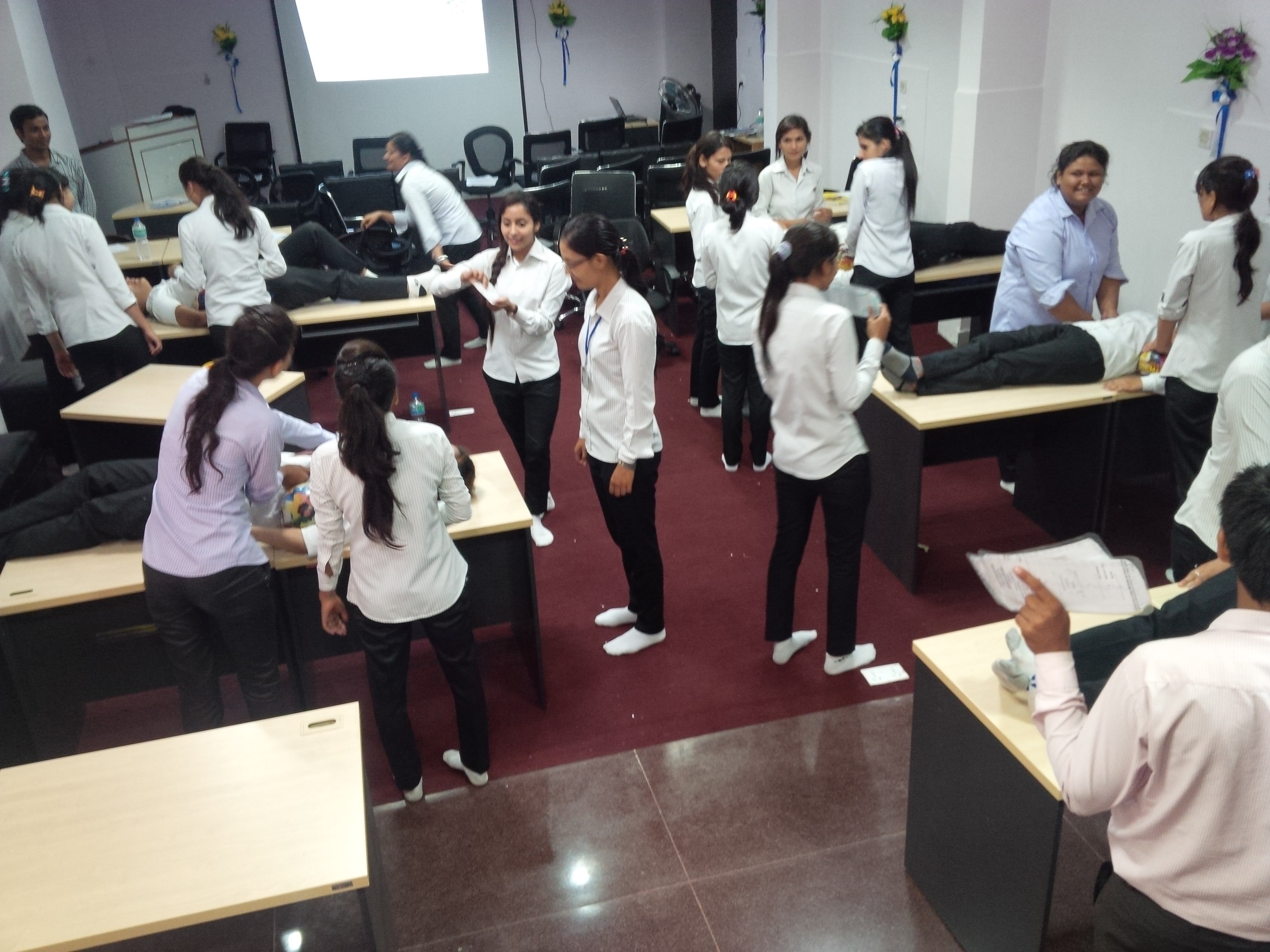





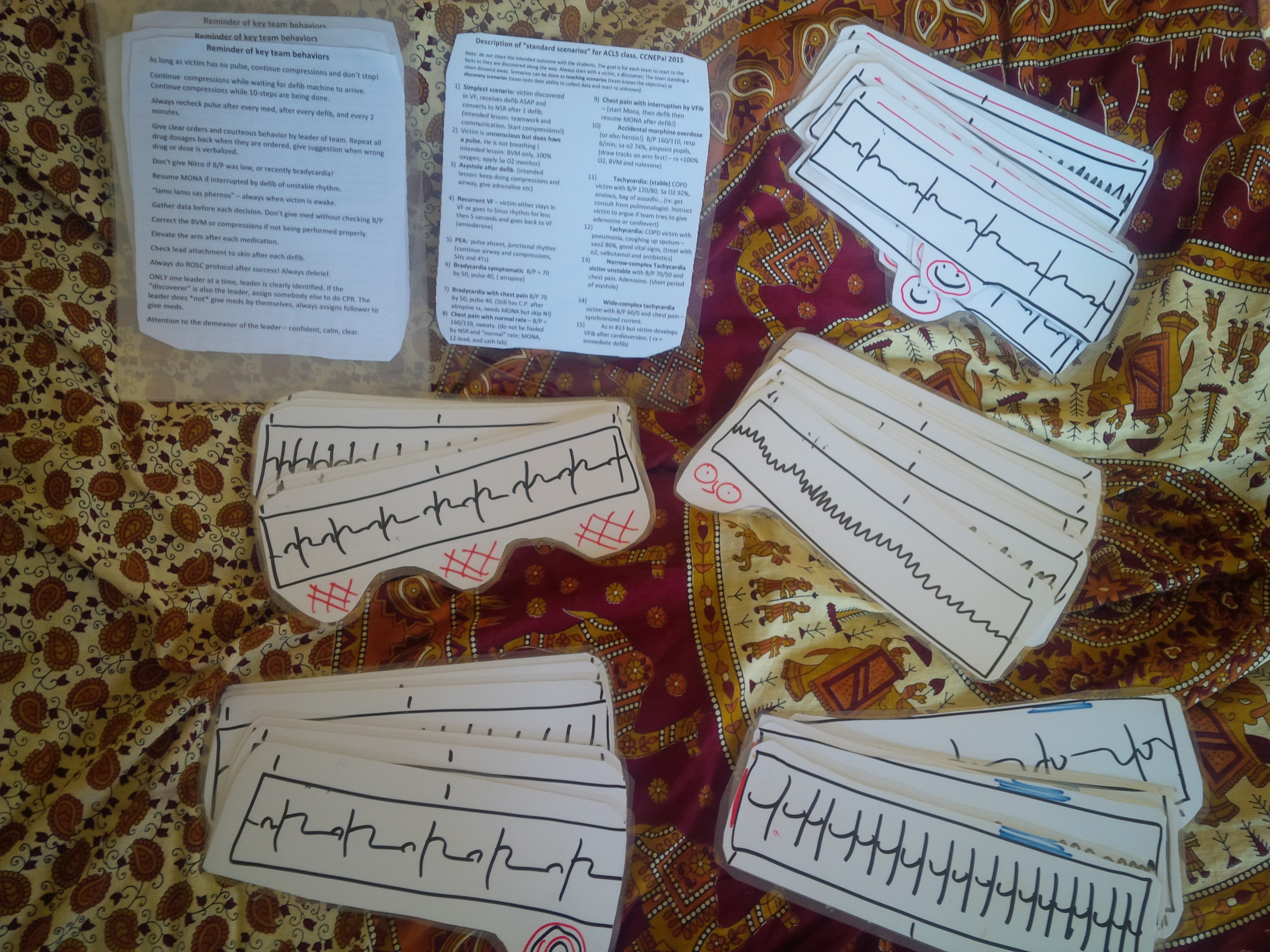


 I always teach as much of the latest protocols as I can, though the American curriculum needs to be adapted to reflect things like the availability of drugs and equipment. I get the protocols from the American Heart Association and this year I got all the bells and whistles – the complete “Instructor Package” including books DVDs and posters.
I always teach as much of the latest protocols as I can, though the American curriculum needs to be adapted to reflect things like the availability of drugs and equipment. I get the protocols from the American Heart Association and this year I got all the bells and whistles – the complete “Instructor Package” including books DVDs and posters.







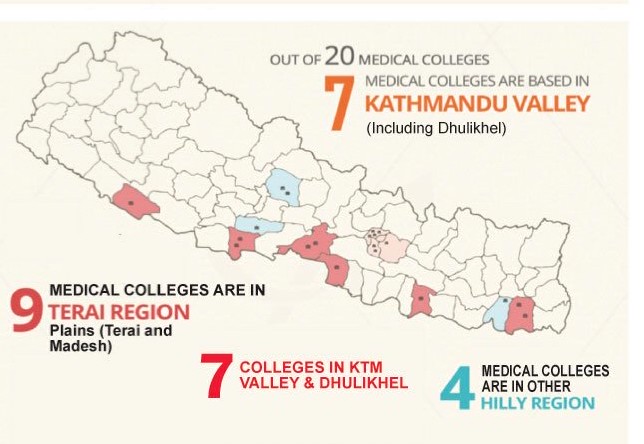
 The male colleagues of this story seem to merit a special bhai tika. sometimes we take this meaning of these ceremonies for granted. Yes, women should stand on their own two feet; but aren’t we all here to help each other?
The male colleagues of this story seem to merit a special bhai tika. sometimes we take this meaning of these ceremonies for granted. Yes, women should stand on their own two feet; but aren’t we all here to help each other? There have been highly publicized episodes of threats and attacks against doctors in Nepal. In September the Cabinet proposed a rule change to put the burden of payment to surviving family firmly on the back of whichever doctor was involved when a patient died. This led the Nepal Medical Association to protest, and hospitals in Nepal were closed for a week this past September. The cabinet decided to delay implementing any new rule, and (among other things) a committee was formed to study the issue.
There have been highly publicized episodes of threats and attacks against doctors in Nepal. In September the Cabinet proposed a rule change to put the burden of payment to surviving family firmly on the back of whichever doctor was involved when a patient died. This led the Nepal Medical Association to protest, and hospitals in Nepal were closed for a week this past September. The cabinet decided to delay implementing any new rule, and (among other things) a committee was formed to study the issue. the
the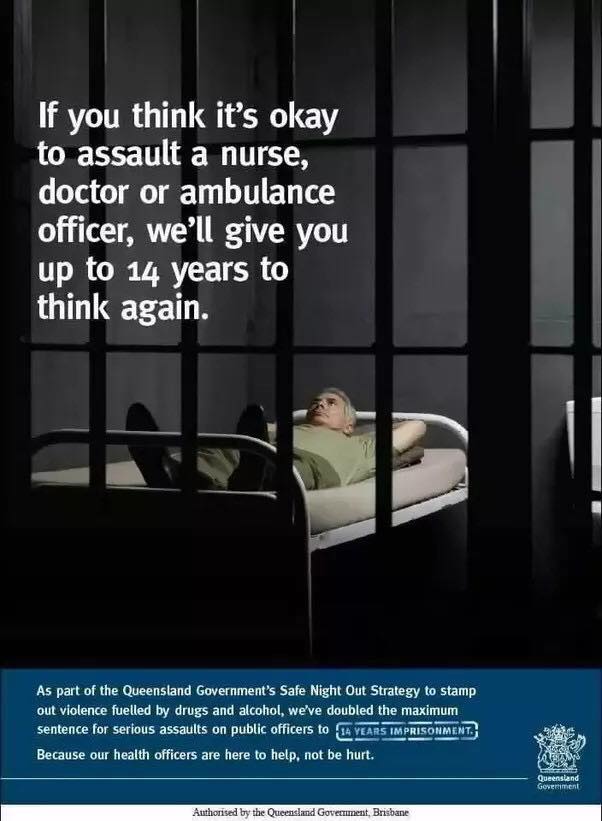







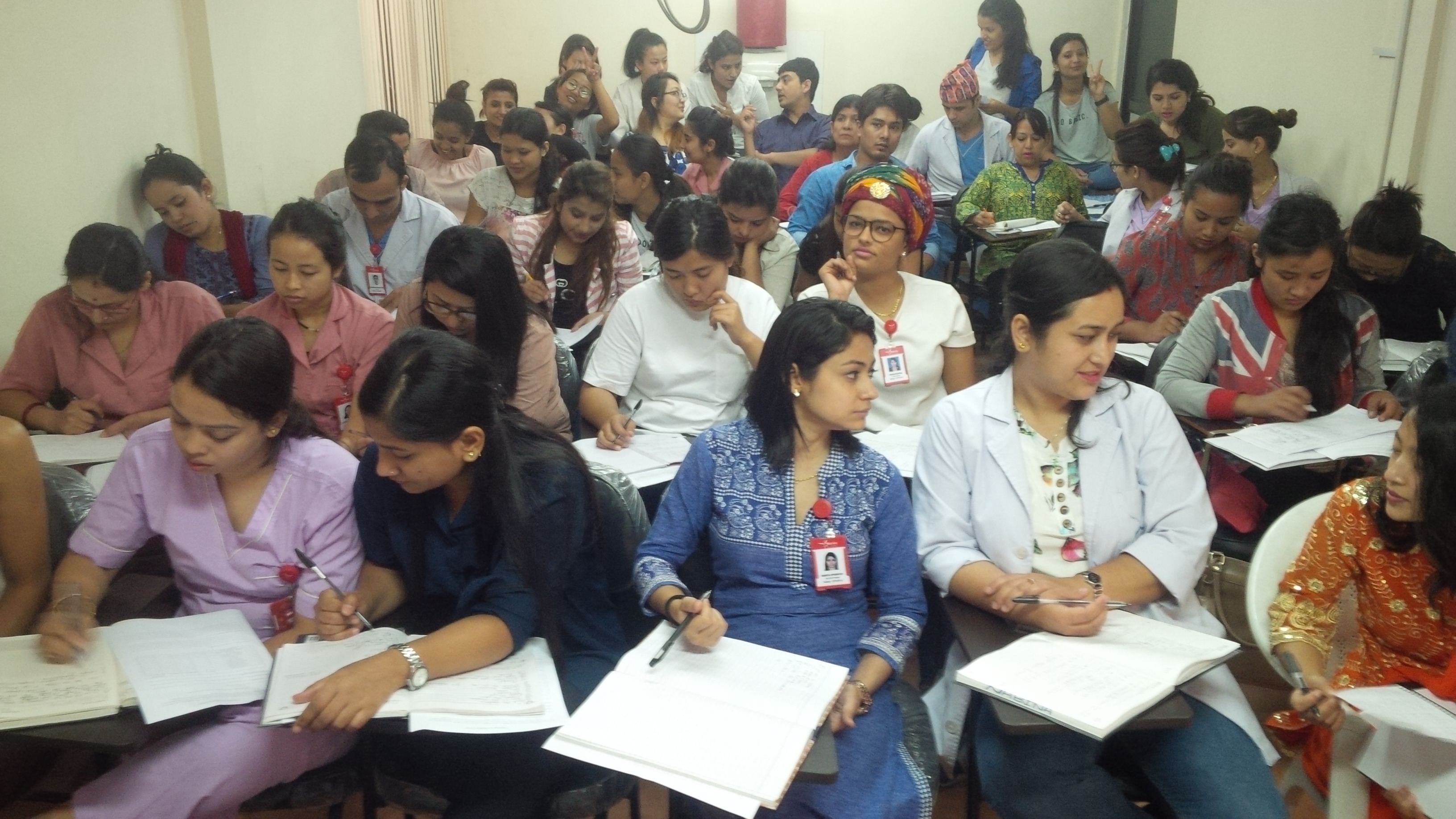

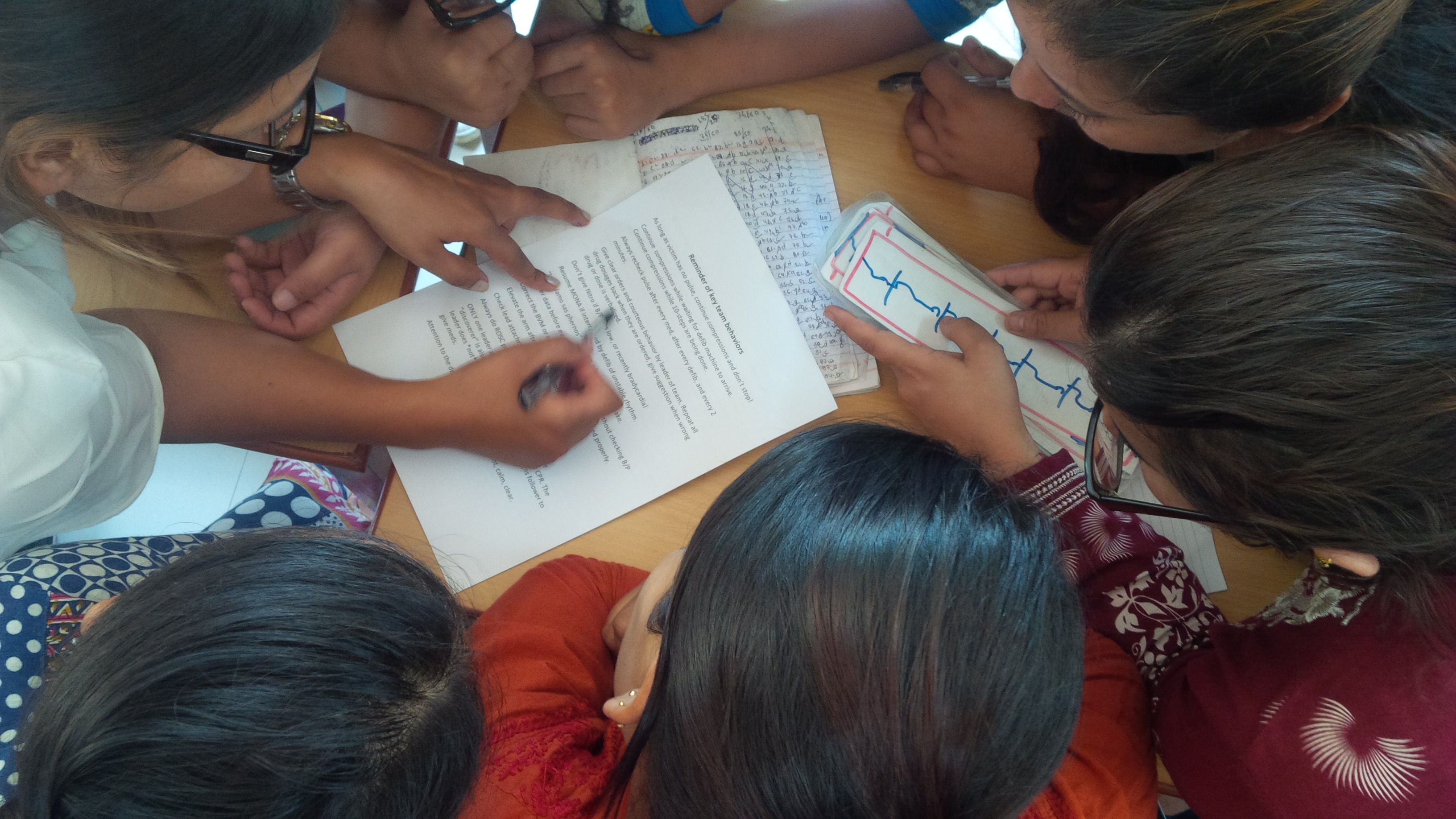

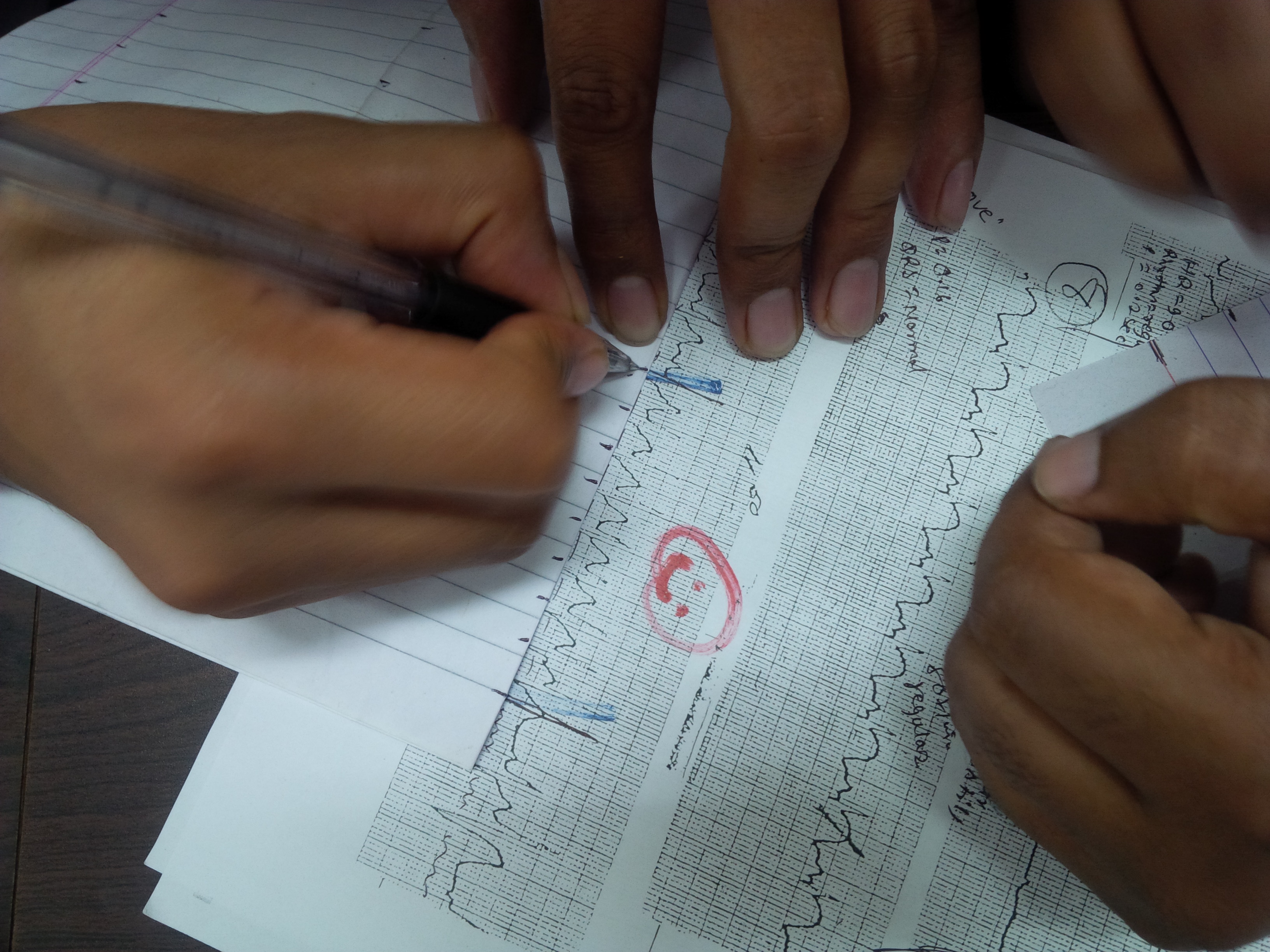




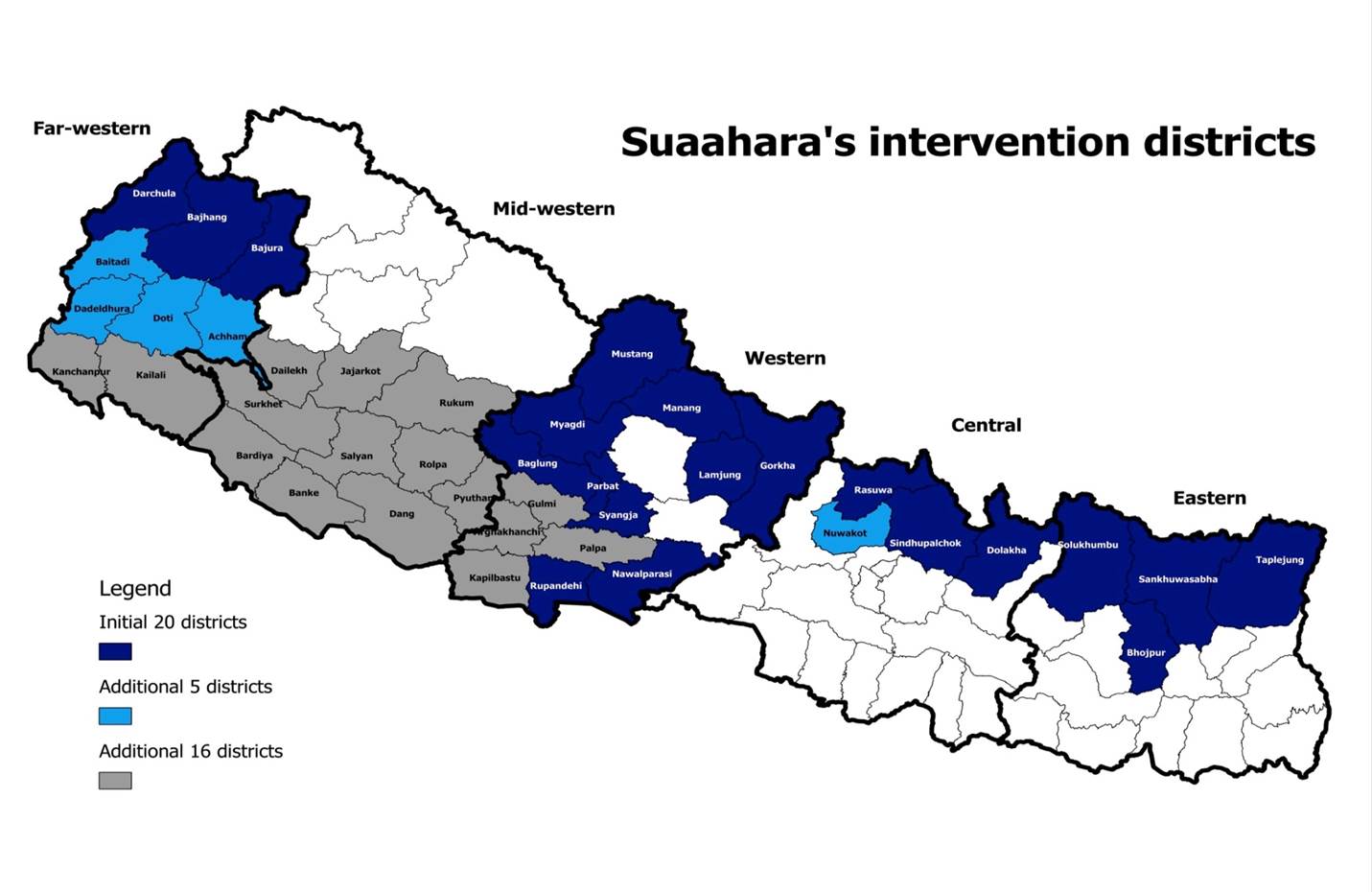
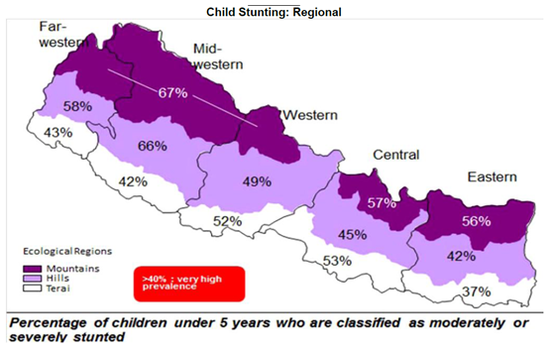

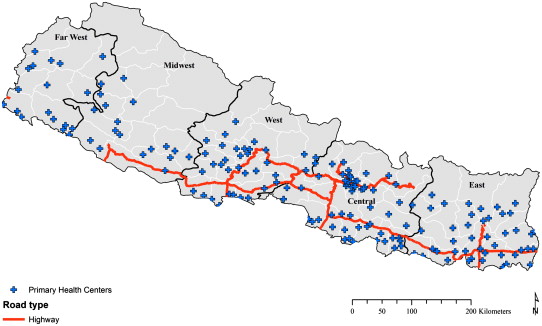




 Summer 2017 CCNEPal will once again teach in Nepal.
Summer 2017 CCNEPal will once again teach in Nepal.